
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Successful sequential extracorporeal multiple organ support therapy in COVID-19 pneumonia: A case report
Cynthia Estefanía Villasana Salazar1; Cynthia Isabel Ortiz López1; Jorge Alberto Hernández Portales1,2; Alicia Esthela López Romo1,3; Lilia María Rizo Topete1,4,5*
1 Internal Medicine, Christus Muguerza, Universidad de Monterrey, Monterrey, Nuevo León, México.
2 Neumology and Critical Care, Christus Muguerza, Universidad de Monterrey, Monterrey, Nuevo León, México.
3 Infectology, Christus Muguerza, Universidad de Monterrey, Monterrey, Nuevo León, México.
4 Nephrology, Christus Muguerza, Universidad de Monterrey, Monterrey, Nuevo León, México.
5 Nephrology, Hospital Universitario “José Eleuterio González”, UANL, Monterrey, Nuevo León, Mexico.
*Corresponding Author: Lilia María Rizo-Topete
Nephrology, Christus Muguerza, Universidad de Monterrey, Andes #2707 Obispado, Monterrey, Nuevo León,
64050, Mexico.
Email: marili18@hotmail.com
Received : Nov 05, 2021
Accepted : Dec 27, 2021
Published : Jan 03, 2021
Archived : www.jcimcr.org
Copyright : © Rizo-Topete LM (2021).
Abstract
Patients with severe COVID-19 pneumonia can develop acute respiratory distress syndrome, which triggers respiratory failure. Multiple Organ Support Therapies (MOST), such as Extra Corporeal Membrane Oxygenation (ECMO), Continuous Renal Replacement Therapy (CRRT) or plasmapheresis, can be used as part of adjunctive management in patients with refractory hypoxemia even with the appropriate use of optimal mechanical ventilation and pharmacological measures. We describe a case of a 31-year-old man who, upon admission, is managed with mechanical ventilation and due to poor evolution, it is decided to start ECMO therapy within the first 24 hours of admission; subsequently, management with CRRT with oXiris filter and plasmapheresis is initiated in the first three days of hospitalization. The patient presents a rapid clinical improvement and a significant decrease in inflammatory markers. CRRT with oXiris filter has been associated with a significant reduction in cytokine and endotoxin levels; while plasmapheresis therapy also eliminates inflammatory mediators. Management with ECMO has shown benefits as salvage therapy in patients with hypoxemia. The success of these cases depends largely on the early onset of ECOS in the critically ill patient.
Keywords: COVID-19; CRRT; ECMO; MOST; oXiris.
Citation: Salazar CEV, López CIO, Portales JAH, Romo AEL, Topete LMR, et al. Successful sequential extracorporeal multiple organ support therapy in COVID-19 pneumonia: A Case Report. J Clin Images Med Case Rep. 2022; 3(1): 1529.
Introduction
Among the laboratory findings of COVID-19 we encounter inflammatory markers elevation. In the management of severe cases of pneumonia, the use of protective mechanical ventilation combined with a prone position and adequate pharmacological management is key; however, in many patients this is not enough to avoid severe hypoxemia. In these cases, extracorporeal support therapies can be used to seek improvement in the organ function of the patient [1-3].
Case report
A 31-year-old man with morbid obesity (BMI 55) is admitted due to respiratory failure with a 7-day evolution characterized by fever, malaise and progressive dyspnea. Upon arrival, he presented tachycardia, tachypnea and fever, O2 saturation in 83% with a PaO2 / FiO2 of 52. PCR was requested for Covid-19 with a positive result and a chest CT scan resulting in CO-RADS 5. He was treated with acetaminophen, azithromycin, enoxaparin and dexamethasone. High-flow nasal canula was placed however low O2 saturation and tachypnea persisted; Mechanical Ventilation (IMV) with orotracheal intubation was applied. Due to poor evolution and hypoxemia, it was decided to start ECMO therapy within 12 hours after the start of IMV. At 48 hours after admission, CRRT was started with HDFVVC modality with prismaflex and oXiris filter. At 72 hours, 5 sessions of plasmapheresis were indicated with extraction of 4000cc plus infusion of albumin. A significant decrease in inflammatory markers was documented (Table 1) as well as evident clinical improvement, so it was decided to withdraw ECMO and CRRT on the fourth day of admission. On the fifth day of admission IMV was withdrawn andhe was discharged from the ICU a week after admissionand finally discharged home on day 18 of hospital stay.
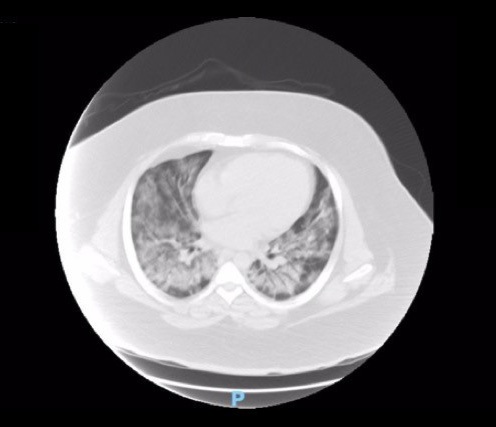

Table 1:Laboratory markers progression during MOST.
|
IMV |
IMV |
IMV |
IMV |
IMV |
Plasmapheresis |
|
Day 1 |
Day 2 |
Day 3 |
Day 4 |
Day 5 |
Day 6 |
Hemoglobin |
14.3 |
13.7 |
11.4 |
10.1 |
- |
9.6 |
Leukocytes |
8.52 |
10.09 |
5.88 |
9.16 |
- |
10.64 |
Lymphocytes |
0.44 |
0.56 |
0.57 |
0.60 |
- |
1.01 |
Creatinine |
0.82 |
0.83 |
3.01 |
2.59 |
1.08 |
1.29 |
BUN |
11.8 |
16 |
43.9 |
40.7 |
17.7 |
21.7 |
Alkalinephosphatase |
94 |
85 |
60 |
52 |
- |
26 |
LDH |
903 |
1126 |
1087 |
897 |
- |
487 |
C-reactive protein |
207.36 |
205.65 |
- |
57.3 |
- |
- |
Interleukin 6 |
- |
- |
- |
505.7 |
167.5 |
177 |
Discussion
The clinical deterioration of patients with COVID-19 is believed to be due to a state of inflammation; it has been reported that patients with severe SARS-CoV-2 infection have an elevation of pro-inflammatory cytokines such as interferon, interleukins (IL-1B, IL-6, IL-12) and chemokines (CXCL10 and CCL2) that are associated with inflammation [4,5].
In severe cases of COVID-19, Multiple Organ Support Therapies (MOST) are the main treatment; one of the most used is CRRT. Hemofilters used for the adsorption of endotoxins and inflammatory cytokines, specially oXiris filter with its extracorporeal purification capacity, has been associated with a significant decrease in cytokine and endotoxin levels compared to other filters, which leads to an improvement in hemodynamic status with a decrease in the requirement for vasopressor management [6-10].
Also, plasmapheresis is another extracorporeal therapy that selectively removes plasma with large molecules and subsequently replaces it with fresh frozen plasma or albumin. Therefore, it improves organ function by eliminating inflammatory mediators and antifibrinolytic substances.
ECMO therapy has been proposed as salvage therapy in patients with severe hypoxemia despite support with IMV. When the patient presents PaO2 / FiO2 figures <100 mmHg or uncompensated respiratory acidosis for more than 6 hours after the use of IMV, the use of ECMO should be considered [11].
Conclusion
Although there is still a high mortality in ARDS secondary to COVID-19 even after management with extracorporeal support therapies, these could be the best chance of improvement for patients with refractory hypoxemia to IMV. Starting them at the most opportune time, as in our case, is key to their success. This type of therapy could be an integral part of the management of critical patients with COVID-19 pneumonia or other acute pathologies with a high inflammatory load.
Statement of ethics: Written informed consent to publish this case report has been given to us by the patient.
Informed consent: Consent form obtained from patient and sent to journal editorial office.
Conflict of interest statement: There are no conflicts of interest.
Funding sources: There are no funding sources.
Author contributions: CEVS, CIOL, LMRT and JAHP developed the idea, design and directed the realization of this case report. LMRT, JAHP and AELR helped supervise the project. CEVS and CIOL gather the patient’s data, research for bibliography and wrote the manuscript. All authors provided critical feedback and helped shape the manuscript.
Data availability statement: The data that support the findings of this manuscript are not publicly available due to containing information that could compromise the privacy of the participant but are available from the corresponding author upon reasonable request.
References
- Guan W J, Ni Z Y, Hu Y, Liang W H, Ou C Q, He J X, et al. Clinical characteristics of Coronavirus disease 2019 in China. N Engl J Med. 2020; 382: 1708–1720.
- COVID-19 map johns Hopkins Coronavirus resource Center. Jhu. edu. 2021. Available from: https://coronavirus.jhu.edu/map. html
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel Coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020; 382: 727–733.
- Ye Q, Wang B, Mao J. The pathogenesis and treatment of the `Cytokine Storm’ in COVID-19. J Infect. 2020; 80: 607–613.
- Coperchini F, Chiovato L, Croce L, Magri F, Rotondi M. The cytokine storm in COVID-19: An overview of the involvement of the chemokine/chemokine-receptor system. Cytokine Growth Factor Rev. 2020; 53: 25–32.
- Chu KH, Tsang WK, Tang CS, Lam MF, Lai FM, To KF, et al. Acute renal impairment in coronavirus-associated severe acute respiratory syndrome. Kidney Int. 2005; 67: 698–705.
- Schwindenhammer V, Girardot T, Chaulier K, Grégoire A, Monard C, Huriaux L, et al. OXiris® use in septic shock: Experience of two french centres. Blood Purif. 2019; 47 Suppl 3: 1–7.
- Constantinescu C, Pasca S, Tat T, Teodorescu P, Vlad C, Iluta S, et al. Continuous renal replacement therapy in cytokine release syndrome following immunotherapy or cellular therapies? J Immunother Cancer. 2020; 8: e000742.
- Shum HP, Chan KC, Kwan MC, Yan WW. Application of endotoxin and cytokine adsorption haemofilter in septic acute kidney injury due to Gram-negative bacterial infection. Hong Kong Med J. 2013; 19: 491–497.
- Broman ME, Hansson F, Vincent J-L, Bodelsson M. Endotoxin and cytokine reducing properties of the oXiris membrane in patients with septic shock: A randomized crossover double-blind study. PLoS One. 2019; 14: e0220444.
- Li Y, Liu S, Zhang S, Ju Q, Zhang S, Yang Y, et al. Current treatment approaches for COVID-19 and the clinical value of transfusionrelated technologies. Transfus Apher Sci. 2020; 59: 102839.