
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Prolonged bronchoscopy in a case of multiple level central airway obstruction: A case report
Priyanka Mishra*; Revanth Challa; Debender Tripathy
Department of Anaesthesia and Critical Care, AIIMS Rishikesh, India.
*Corresponding Author: Priyanka Mishra
Department of Anaesthesia and Critical Care, AIIMS
Rishikesh, India.
Email: pmishra15390@gmail.com
Received : Nov 06, 2021
Accepted : Dec 27, 2021
Published : Jan 03, 2022
Archived : www.jcimcr.org
Copyright : © Mishra P (2022).
Abstract
Bronchoscopy poses distinct challenges for anaesthesia as the airway is shared by both the surgeon and anaesthetist. This difficulty increases manifold when the obstruction is present simultaneously in both the trachea and bronchi. The individualized anaesthetic approach is governed by the location and nature of obstruction along with airway size at the obstruction site. We present a case of 50 years old male, with partial tracheal and complete right bronchial obstruction posted for bronchoscopy. We successfully managed this case of unanticipated prolonged bronchoscopy. Anaesthesia was maintained by total intravenous anaesthesia and spontaneous assisted ventilation without intubation and muscle relaxation.
Keywords: airway obstruction; anesthesia; bronchoscopy; tracheobronchial growth.
Citation: Mishra P, Challa R, Tripathy D. Prolonged bronchoscopy in a case of multiple level central airway obstruction: A case report. J Clin Images Med Case Rep. 2022; 3(1): 1530.
Introduction
Bronchoscopy poses distinct challenges for anesthesia as the airway is shared by both surgeon and anaesthetist. This difficulty increases manifold when the obstruction is present in both the trachea and bronchi. The anaesthetic approach is governed by the location of the obstruction, airway size at the obstruction site, and the nature of obstruction (fixed or dynamic and pedunculated or polypoidal). We present a case of successful management of an unanticipated prolonged rigid bronchoscopy in a patient with partial tracheal and complete right bronchial obstruction.
Case report
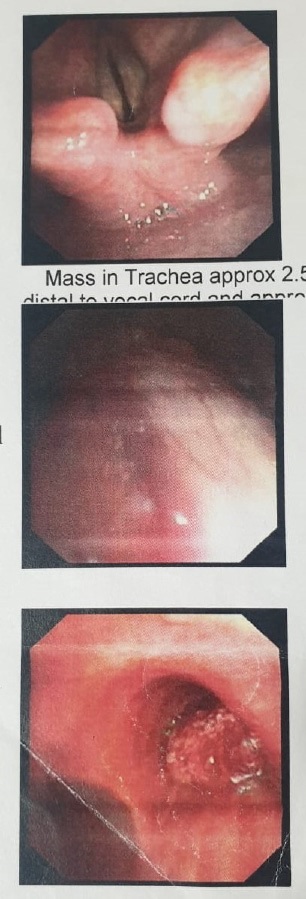
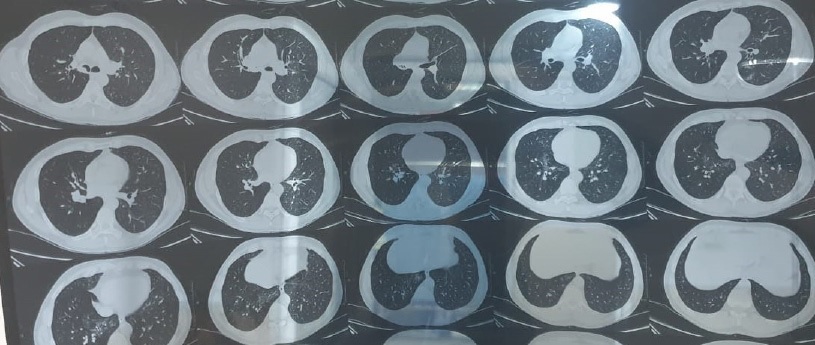
A 50-year-old, Hepatitis C positive male patient, weighing 54 kg was posted for diagnostic and therapeutic bronchoscopy. He was a known case of Chronic Obstructive Pulmonary Disease (COPD) and had presented with complaints of progressive dyspnea and hemoptysis. The pre-anaesthetic evaluation showed Medical Research Council (MRC) grade three dyspnea. Flow– volume loop revealed fixed extrathoracic obstruction. Aortogram and bronchoscopy showed 2.5 X 2.0 cm polypoidal lesion in cervical trachea and 3.0 X 2.3 cm lesion in right main bronchus causing complete luminal narrowing (Figure 1 and 2). Air trapping and pneumonia were also seen in the right lung. The rest of the investigations were within normal limits. The patient was shifted into the operating room (OR) and all the standard monitors were attached. Baseline parameters were recorded as heart rate – 76/min, Blood Pressure (BP)–136/88 mmHg, and on-air oxygen saturation (spO2 ) of 97%. Intravenous (IV) access was secured with 18 gauge cannula in the left hand. Premedication was done with injection glycopyrrolate and midazolam IV and salbutamol nebulization. As the tracheal lumen was narrowed down to nearly half, it was decided to proceed with the procedure without intubation, using spontaneous assisted ventilation. After pre-oxygenation with 100% oxygen for three minutes, induction of anaesthesia was done with 150 mg propofol and 100 mcg fentanyl. Lignocaine 2% IV was given to prevent the sympathetic response to bronchoscopy. The patient was then handed over to a pulmonologist. Anaesthesia was maintained with propofol infusion at 100 mcg/kg/min and fentanyl aliquots. Intermittent high flow oxygen was provided through the side port of the bronchoscope and adequate ventilation was assessed by chest movements. After the resection of polypoidal tracheal growth, there was a decrease in airway resistance from 32 mmHg earlier to 28 mmHg. Inj. dexamethasone 8 mg IV was given to reduce swelling and inflammation. The depth of anaesthesia was continuously monitored by hemodynamic parameters and respiration. Capnography could not be measured. This was followed by fibreoptic bronchoscopy for assessing bronchial obstruction. Topical anaesthesia was provided by spraying 4% lignocaine while advancing to prevent laryngospasm. A combination of electrocautery, laser, and cryotherapy was used to resect the fungating bronchial growth. During these periods, oxygen flow was discontinued to avoid the risk of airway fire. There was the intra-operative finding of the bronchial growth involving a longer segment (3 cm) of the right main bronchus than was expected. The repeated attempts to remove the fungating growth lead to increased bleeding. This was accompanied by a brief period of desaturation such that spO2 dropped to 71%. After control of bleeding, adequate suctioning of both right and left bronchi was done. Finally, patency was achieved in the bronchial lumen to reveal the purulent material of pneumonia, which was suctioned out. The total duration of the procedure was 120 minutes. At the end of the procedure, propofol infusion was stopped and after complete arousal of the patient with the ability to maintain airway, he was transferred to the post-anaesthesia care unit. The same day later, he was discharged from the hospital.
Discussion
Rigid bronchoscopy demands a meticulous anaesthetic strategy that needs to be tailored as per the case specifications. Preanaesthetic evaluation plays a vital role in the assessment of individual risks and adequate optimization. Airway narrowing due to intraluminal or extraluminal tracheal/bronchial compression makes airway management difficult and also produces difficulties in ventilation [1]. In our case, there was a polypoidal fixed tracheal growth and fungating growth at the right main bronchus causing complete occlusion of the bronchial lumen. The challenge lied in providing the ideal cocktail of adequate analgesia, hypnosis, and muscle relaxation for the procedure while maintaining ventilation. Pre-medication should be done with antisialogogue agents like atropine and glycopyrrolate to reduce the amount of secretions. We also gave pre-operative salbutamol nebulization to achieve bronchodilation and improve pulmonary function. Specific considerations for anaesthetic agents in bronchoscopy include the requirement for rapid and complete recovery to allow full return to baseline respiratory function as these patients have marginal respiratory status [2]. The drugs that can be used to provide sedation include Benzodiazepines (midazolam, lorazepam and diazepam), opiods (fentanyl, remifentanyl), propofol, Fospropofol, ketamine and dexmedetomidine. Though ketamine is a potent bronchodilator and analgesic, it does not attenuate the upper airway reflexes and increases salivation and secretions. Hence, we used propofol with fentanyl for induction and maintenance of anaesthesia over inhalational anaesthesia as delivery of inhalational agent must have been interrupted with discontinued ventilation while suctioning, dilation of bronchus, or stent placement. Target controlled infusion can be employed as a part of TIVA. Muscle relaxant was not used as there was a risk of total airway collapse. The various ventilation strategies employed for bronchoscopy include apnoeic oxygenation, Spontaneous assisted ventilation, Controlled ventilation, Manual jet ventilation, and High-frequency jet ventilation [3]. As our patient was a case of COPD with evidence of air trapping, jet ventilation was ruled out owing to the risk of bulla rupture leading to pneumothorax. The patient had nearly 50% tracheal lumen obstruction at 2 cm distal to vocal cords and hence, it was not feasible to intubate the trachea while allowing for bronchoscopy instrumentation. Moreover, any attempt at intubation could have resulted in the breakage of this growth which could have displaced further and made ventilation more difficult. Hence, we decided to proceed with spontaneous assisted ventilation without intubation and provided 100% oxygen through the bronchoscope, considering the leaks and intermittent breaks. The intra-operative finding of a longer segment of occluding growth in the right main bronchus prolonged the procedure than expected. The various complications associated with bronchoscopy include hypoxia, hemorrhage, hemodynamic instability, congestion due to secretions and tissue fragments, pneumothorax, perforation, air embolism, laryngospasm, and bronchospasm [3]. Special caution should be taken to avoid airway fires while use of laser and cautery by reducing inspired oxygen fraction to <o.5 [4]. Emergence should be smooth so as to avoid any complications. Corticosteroids can be given to avoid airway edema and inflammation.
Conclusion
Bronchoscopy for obstructions at multiple levels in airwaycan present unique challenges for the anaesthetist. However, detailed pre-operative assessment, planning of individualized anaeshetic approach can significantly improve the patient prognosis.
Highlights
Bronchoscopy in the presence of both tracheal and bronchial obstruction is an anaesthetic challenge. • There was 2.5 X 2.0 cm polyopidal lesion in cervical trachea and 3.0 X 2.3 cm lesion in right main bronchus. • Anaesthesia was maintained by total intravenous anaesthesia and spontaneous assisted ventilation without intubation and muscle relaxation. • Complications include hypoxia, haemorrhage, laryngospasm, bronchospasm and airway fires.
References
- Goudra BG, Singh PM, Borle A, et al. Anesthesia for Advanced Bronchoscopic Procedures: State-of-the-Art Review. Lung. 2015; 193: 453-465.
- Pathak V, Welsby I, Mahmood K, et al. Ventilation and anesthetic approaches for rigid bronchoscopy. Ann Am Thorac Soc. 2014; 11: 628–634.
- Chadha M, Kulshrestha M, Biyani A. Anaesthesia for bronchoscopy. Indian J Anaesth. 2015; 59: 565-573.
- Eichhorn JH, Eisenkraft JB. Expired oxygen as the unappreciated issue in preventing airway fires: Getting to “never” Anesth Analg. 2013; 117: 1042–1044.