
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Liver lesion characterization in a patient with cirrhosis due to cardiac congestion: Limitations of LI-RADS
Tejal Gapchup1; Constantine Burgan2; Kristin K Porter2*
1 Maharashtra Institute of Medical Education and Research (MIMER) Medical College, Talegaon Dabhade, Pune, India.
2 Department of Radiology, University of Alabama at Birmingham, Birmingham, Alabama, USA.
*Corresponding Author: Kristin Porter
Department of Radiology, University of Alabama at
Birmingham, 619 19th Street South, Birmingham, AL
35249, USA.
Email: kkporter@uabmc.edu
Received : Nov 09, 2021
Accepted : Dec 30, 2021
Published : Jan 06, 2022
Archived : www.jcimcr.org
Copyright : © Porter K (2022).
Abstract
The MRI findings of a liver lesion in a patient with congenital heart disease are presented and the differences between the two types of MR contrast agents, i.e., extracellular and intracellular (hepatobiliary), and their role in characterizing the imaging features of hepatocellular carcinoma are discussed. The diagnostic algorithm of LI-RADS cannot be used to characterize liver lesions in patients with cardiac cirrhosis (secondary to congestive hepatopathy following congenital heart disease). The main reason for this is the increased likelihood of the presence of confounding benign lesions resulting from chronic hepatic congestion. The only definitive way to diagnose suspicious liver lesions in these patients is the histopathological examination of these lesions. Hence, there is a need for a new diagnostic imaging algorithm in such patients, which can provide a non-invasive method to identify potentially malignant lesions.
Keywords: CT/MRI LI-RADS; CEUS LI-RADS; gadolinium contrast; MRI contrast agents; congenital heart disease; contrast enhanced ultrasound.
Citation: Gapchup T, Burgan C, Porter KK. Liver lesion characterization in a patient with cirrhosis due to cardiac congestion: Limitations of LI-RADS. J Clin Images Med Case Rep. 2022; 3(1): 1539.
Introduction
Hepatocellular Carcinoma (HCC) is most commonly seen in patients with a background of liver cirrhosis [1]. Standardized imaging tools such as CT/MRI LI-RADS can help categorize liver lesions, guide treatment, and follow-up decisions [2]. However, currently CT/MRI LI-RADS cannot be applied to liver cirrhosis resulting from cardiac congestion, such as in patients with congenital heart disease. In this case report, we describe the MRI findings of a patient diagnosed with liver cirrhosis and known congenital heart disease utilizing both hepatobiliary (intracellular) and extracellular Gadolinium-Based Contrast Agents (GBCA). Since this patient’s cirrhosis was due to cardiac congestion, we could not apply CT/MRI LI-RADS to categorize the liver lesion.
Case presentation
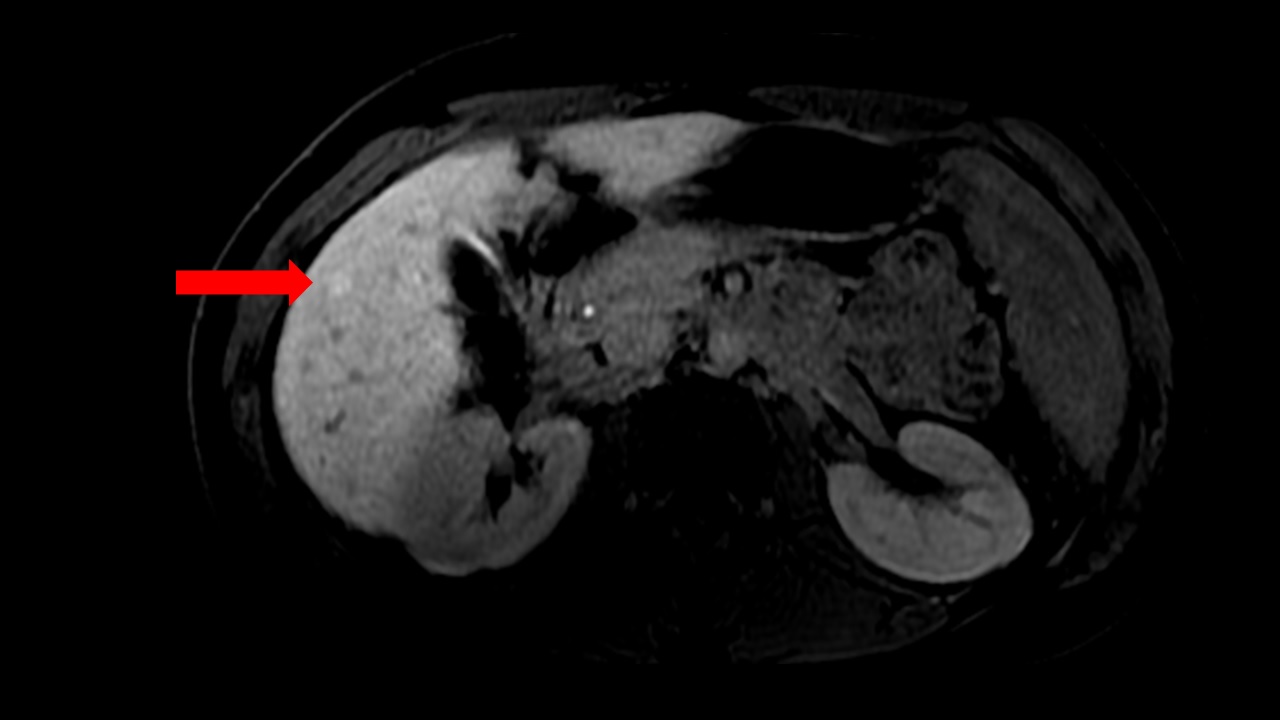
This is a case of a 33-year-old female, with a known history of cirrhosis secondary to hepatic congestion (resulting from sequelae of a single outlet ventricle), (Figure 1), who presented to the hospital for Hepatocellular Carcinoma (HCC) surveillance. The serum alpha-fetoprotein level in this patient was 2.5 ng/ml and had been relatively stable across multiple years.

Imaging findings
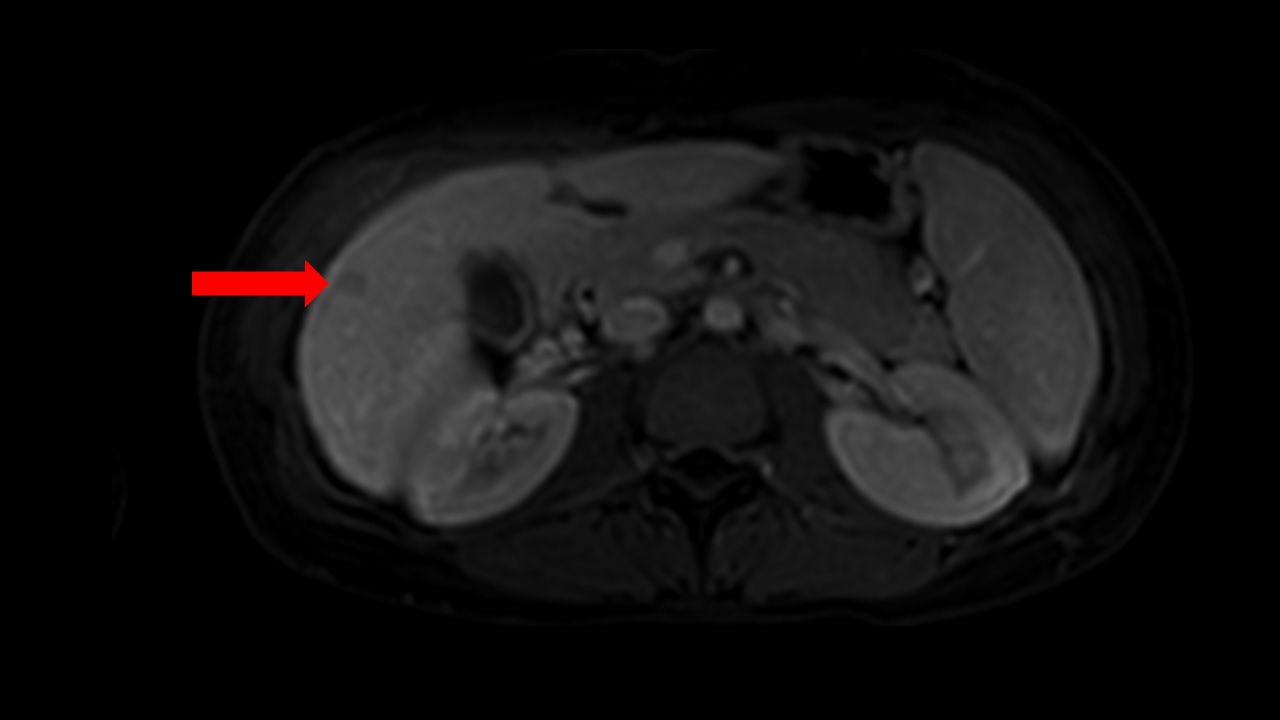
The patient had undergone imaging with hepatobiliary contrast MRI three months prior to the current imaging. This prior scan showed a well-defined, rounded 1.5 cm arterial phase hyperenhancing lesion in the right lobe of the liver, located peripherally in segment five of the liver (Figure 2). The lesion did not exhibit washout in the transition phase and retained contrast on the hepatobiliary phase (Figure 3). These findings suggested a liver lesion with functional hepatocytes, such as well-differentiated HCC.

During a follow up visit, the patient underwent HCC screening with an MRI with an extracellular contrast agent (Gadoteridol). This imaging showed a 1.5 cm hyperenhancing lesion in the arterial phase, with washout during the portal venous and equilibrium phases (Figure 4). These findings would be consistent with a LI-RADS LR 5 lesion (definitely hepatocellular carcinoma); however, given the known diagnosis of congenital heart disease, the use of CT/MRI LI-RADS and CEUS LI-RADS to characterize the liver lesion is precluded.
Discussion
Imaging features of HCC on MRI
The Liver Imaging Reporting and Data System (LI-RADS) is a standardized tool for the interpretation and reporting of liver imaging findings. It provides uniform algorithms for each of the various imaging modalities to categorize liver lesions on a spectrum from benign to malignant in patients at high risk for HCC. The various imaging modalities used in LI-RADS for the purpose of surveillance, diagnosis and staging of HCC are CT, MRI (with extracellular and hepatobiliary contrast agents), Ultrasonography (US) and Contrast Enhanced Ultrasonography (CEUS) [2].
The Liver Imaging Reporting and Data System (LI-RADS) is a standardized tool for the interpretation and reporting of liver imaging findings. It provides uniform algorithms for each of the various imaging modalities to categorize liver lesions on a spectrum from benign to malignant in patients at high risk for HCC. The various imaging modalities used in LI-RADS for the purpose of surveillance, diagnosis and staging of HCC are CT, MRI (with extracellular and hepatobiliary contrast agents), Ultrasonography (US) and Contrast Enhanced Ultrasonography (CEUS) [2].
If a lesion is hypointense on the hepatobiliary phase (not functional and potentially more suspicious for malignancy) but is also not showing washout nor arterial phase enhancement (arterial blood supply of the tumor increases during hepatocarcinogenesis, which leads to arterial phase enhancement and hence confers a higher LI-RADS score) it would more likely be malignant. Hence, when we are trying to determine the malignant potential of a new liver lesion, the functionality of that liver lesion takes precedence over its vascularity. New malignant lesions may not have a welldeveloped vascular system and may be missed on arterial phase, but their lack of functionality will be detected during the hepatobiliary phase of MRI [4].
Characterizing indeterminate liver lesions in a patient with cirrhosis due to cardiac congestion: Beyond LI-RADS
Each of the imaging modalities in LI-RADS has specific inclusion and exclusion criteria. For example, CT/MRI diagnostic LI-RADS is designed for patients who are at a high risk of HCC, including patients with cirrhosis, chronic hepatitis B infection, patients with prior HCC and adult liver transplant candidates and recipients. The causes of cirrhosis are also well defined in the algorithm. Liver cirrhosis resulting from alcohol use, hepatitis B infection and Non-Alcoholic Fatty Liver Disease (NASH) are included in the screening protocol. However, CT/MRI LI-RADS does not apply to cirrhosis resulting from vascular disorders such as hereditary hemorrhagic telangiectasia, Budd-Chiari syndrome, chronic portal vein occlusion, or cardiac congestion [2].
Patients with congenital heart disease may develop right heart failure, contributing to hepatic congestion. Chronic hepatic congestion increases the risk of development of benign hyperplastic nodules that may resemble HCC on imaging, potentially causing false positive diagnoses [2]. This may lead to diagnostic inaccuracies on imaging, as both have similar radiologic features, ie arterial phase enhancement, when viewed on contrast MRI. Hence, use of LI-RADS (for MRI and CEUS features) may prove challenging in establishing an accurate diagnosis of HCC in a patient with congenital heart disease [5].
Even though the diagnostic criteria for HCC using LI-RADS cannot be applied in this patient population (due to potential confounding with the commonly present benign lesions), surveillance for HCC is still advised using the same modalities [6]. The presence of any suspicious findings on surveillance can then prompt a biopsy of the lesion, which is currently the only definitive diagnostic tool in these patients.
Options for a patient with indeterminate liver lesion detected on CT/MRI LI-RADS at present include Contrast-Enhanced Ultrasound (CEUS), which uses a purely intravascular contrast (microbubbles) agent. This is unlike CT and MRI contrast agents, which also have an interstitial phase in addition to the arterial phase. Moreover, the ultrasound modality allows for continuous acquisition of images and an uninterrupted evaluation of the vascular phases. This can resolve discrepancies that may arise due to arterial phase mistiming and can allow detection of arterial phase enhancing lesions missed on CT or MRI [7,8]. Although CEUS cannot be used for complete HCC staging due to the limited field of view during imaging, it can be used for characterization of focal liver lesions previously identified on MRI/CT [9]. However, at present, CEUS LI-RADS is also limited in this patient population with cirrhosis due to cardiac congestion [10].
Conclusion
There is a need for a definitive imaging modality to characterize liver lesions in patients with cirrhosis secondary to cardiac congestion. The liver lesions in these patients cannot currently be evaluated for HCC using the CT/MRI LI-RADS due to potential confounding with hyperplastic nodules. Although the diagnostic algorithm of LI-RADS cannot be used in this patient population with liver cirrhosis, these patients should undergo regular imaging surveillance to look for any suspicious findings for malignancy and undergo biopsy, if indicated, as histopathological examination of the liver biopsy sample may ultimately be required for definitive diagnosis.
Declarations
Author contributions: TG, CB, and KKP all substantially contributed to the conception and design of the work and the writing and revision of the manuscript. All authors approve the final version of the manuscript and are accountable for its contents.
Conflict of interests: None
References
- Balogh J, Victor D 3rd, Asham EH, et al. Hepatocellular carcinoma: A review. J Hepatocell Carcinoma. 2016; 3: 41-53.
- American College of Radiology. CT/MRI LI-RADS® v2018. https:// www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/ LI-RADS/CT-MRI-LI-RADS-v2018. 2021.
- Golfieri R, Grazioli L, Orlando E, et al. Which is the best MRI marker of malignancy for atypical cirrhotic nodules: Hypointensity in hepatobiliary phase alone or combined with other features? Classification after Gd-EOB-DTPA administration. J Magn Reson Imaging. 2012; 36: 648-657.
- Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part II. Extracellular agents, hepatobiliary agents, and ancillary imaging features. Radiology. 2014; 273: 30-50.
- Asrani SK, Asrani NS, Freese DK, et al. Congenital heart disease and the liver. Hepatology. 2012; 56: 1160-1169.
- Tang A, Hallouch O, Chernyak V, Kamaya A, Sirlin CB, et al. Epidemiology of hepatocellular carcinoma: Target population for surveillance and diagnosis. Abdom Radiol (NY). 2018; 43: 13-25.
- Quaia E. State of the Art: LI-RADS for Contrast-enhanced US. Radiology. 2019; 293: 4-14.
- Wilson SR, Burns PN, Kono Y. Contrast-Enhanced Ultrasound of Focal Liver Masses: A Success Story. Ultrasound Med Biol. 2020; 46: 1059-1070.
- Ferraioli G, Meloni MF. Contrast-enhanced ultrasonography of the liver using Sono Vue. Ultrasonography. 2018; 37: 25-35.
- American College of Radiology. CEUS LI-RAD® v2017 CORE. https://www.acr.org/-/media/ACR/Files/RADS/LI-RADS/CEUSLI-RADS-2017-Core.pdf Published 2017. Accessed November 8, 2021.