
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
May-Thurner syndrome: An uncommon vascular disorder
Jihane EL Mandour*; Jihad Boulaarab; Ouadie EL Menaoui; Meryem Edderai; Hassan Boumedine; Jamal EL Fenni
Radiology Department, Mohammed V Military Hospital, Rabat, Morocco.
*Corresponding Author: Jihane El Mandour
Radiology Department, Mohammed V Military
Hospital, Rabat, Morocco.
Email: jihaneelmandour@gmail.com
Received : Nov 13, 2021
Accepted : Jan 04, 2022
Published : Jan 11, 2022
Archived : www.jcimcr.org
Copyright : © El Mandour J (2022).
Abstract
In 1957, May and Thurner described the iliac vein compression syndrome. This is a disease entity with a variable anatomical state. It’s an anatomical variant that can be congenital or acquired. The mechanical obstruction prevents venous outflow from the LLE, resulting in persistent venous stasis and risk of thrombosis.
Keywords: May-Thurner syndrome; deep vein thrombosis.
Citation: Mandour JEL, Boulaarab J, Menaoui OEL, Edderai M, Boumedine H, et al. May-Thurner syndrome: An uncommon vascular disorder. J Clin Images Med Case Rep. 2022; 3(1): 1546.
Short report
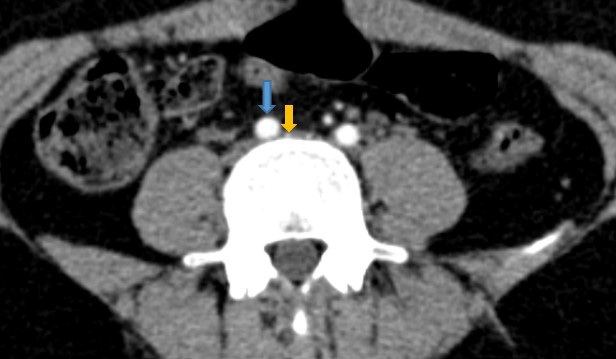
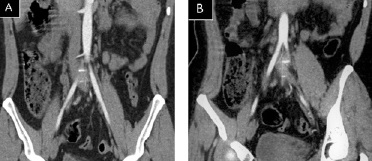
In 1957, May and Thurner described the iliac vein compression syndrome. This is a disease entity with a variable anatomical state [1]. May-Thurner Syndrome (MTS) is a relatively uncommon vascular disorder characterized by constriction of the left common iliac vein, between the right common iliac artery and the lower spine [2] (Figure 1, Figure 2).
MTS is an anatomical variant that can be congenital or acquired [3]. This provides a mechanical barrier to venous flow, increasing the risk of Deep Vein Thrombosis (DVT), chronic venous stasis, and venous hypertension in the Left Lower Extremity (LLE) [3].
The majority of persons with left common iliac vein compression have no symptoms, but MTS can produce symptoms and lead to blood clots called Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) [2].
As a result, some writers advise using the term "May-Thurner anatomy" in patients with no hemodynamic relevance and "May-Thurner syndrome" in cases when the venous flow is restricted and clinical symptoms are present [1].
The mechanical obstruction prevents venous outflow from the LLE, resulting in persistent venous stasis and risk of thrombosis, according to Virchow's triad [3]. Acute DVT chances are increased when other risk factors, such as extended immobilization, obesity, hormonal contraception, and pregnancy, are present [3].
The use of ultrasound in the first-line assessment of a suspected venous compression syndrome is common, however, its sensitivity may be limited above the inguinal plane. Although ultrasound is very reliable for detecting acute iliofemoral DVT, due to their deep placement inside the pelvis, overlaying intestinal gas, obesity, and other factors, examination of the iliac veins is not always possible [1].
The whole amount of iliofemoral venous thrombosis, iliac vein compression, and convoluted venous collaterals can be seen with a CT scan. CT can also be used to rule out other compressive factors such as pelvic masses [1].
Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) are non-invasive and helpful procedures for determining whether a vein is being compressed by an artery [2].
Diagnostic imaging tests should be performed once differential diagnoses have been evaluated to establish the presence of MTS anatomy and decide the appropriate treatment option.
Clinicians should evoke MTS and consider this diagnosis in patients who have unexplained lower limb swelling.
References
- Mako K, Puskas A. May-Thurner syndrome - Are we aware enough? Vasa. 2019; 48: 381-388.
- Liddell RP, Evans NS. May-Thurner syndrome. Vasc Med. 2018; 23: 493-496.
- Yub Raj Sedhai, Reshma Golamari, Aliaksei Salei, Joseph Alukal, Soney Basnyat, et al. May-Thurner Syndrome: Patient Centered Focused Review, The American Journal of the Medical Sciences. http://dx.doi.org/10.1016/j.amjms.2017.09.011.