
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Callus cap over a Küntscher nail: A case report and literature review for heterotrophic ossification
Lavindra Tomar1; Gaurav Govil2*; Pawan Dhawan3
1 Director & Unit Head, Department of Orthopaedics, Max Super Specialty Hospital, Patparganj, Delhi, India.
2 Senior Orthopaedic Consultant, Department of Orthopaedics, Max Super Specialty Hospital, Patparganj, Delhi, India.
3 Attending Orthopaedic Consultant, Department of Orthopaedics, Max Super Specialty Hospital, Patparganj, Delhi, India.
*Corresponding Author: Gaurav Govil
D 101, Sunshine Helios, Sector 78, Noida, Uttar
Pradesh, India – 201304.
Email: gauravgovil@yahoo.co.in
Received : Nov 09, 2021
Accepted : Jan 05, 2022
Published : Jan 12, 2022
Archived : www.jcimcr.org
Copyright : © Govil G (2022).
Abstract
Introduction: Intramedullary Nailing (IMN) has been the gold standard treatment for femoral shaft fractures. Earlier it was managed by Küntscher nail (K nail) fixation. However, in developing countries K nail may still be used as a low-cost fixation device. Heterotrophic Ossification (HO) is a rare complication following nailing in the treatment of femoral shaft fractures. HO along the K nail presenting with late symptomatology have been discussed rarely.
Case report: A 43-year old male presented with a symptomatic callus cap along the proximal end of a left sided femoral K nail. He developed severe pain after a prolonged duration approximating around twenty years of the primary femoral fixation. The hip joint pain intensified with significant limitation affecting daily routine activities. Excision of the smooth contoured callus cap along with the removal of nail was done. The hip function recovered with painless full range of hip motion. There was no evidence of recurrence noted at a twoyear follow-up.
Discussion: The smooth contour of the cap correlated to a persisting HO around the protruding end of K nail with no initial symptoms. The compressive and pressure symptoms along with the callus cap encroachment now contributes to the painful symptoms. The late symptomatology may reasonably be attributed to either impingement or abutment of the callus cap along the pelvic wall.
Conclusion: K nail is an uncommon fixation device for femoral fracture fixation. HO following K nail being another uncommon infrequent complication. The symptomatic acquired HO should be considered for excision to preserve the hip joint function and maintain the ability to do activities of daily living.
Keywords: callus cap; heterotrophic ossification; un-reamed nailing; femur fracture; küntscher nail.
Abbreviations: IMN: Intramedullary Nail; HO: Heterotrophic Ossification; K-nail: Küntscher Nail.
Citation: Tomar L, Govil G, Dhawan P. Callus cap over a küntscher nail: A case report and literature review for heterotrophic ossification. J Clin Images Med Case Rep. 2022; 3(1): 1551.
Introduction
Heterotrophic Ossification (HO) following femoral fracture fixation with IMN have been occasionally reported [1-4]. Callus caps was a term stated by Küntscher for ossified ectopic bone formation in the soft tissues at the prominent proximal end of a nail end at the greater trochanter region [4-6]. A late symptomatic presentation is rarely described.
Removal of callus cap and Intramedullary Nail (IMN) becomes an indication when infection, impingement or management of implant failure requires corrective measures [7]. Removal of HO requires a good pre-operative planning in anticipation of possible complications [8]. More often, removal of any implant presents an unchartered territory with inherent risks of possible complications and scenarios which are implant specific and site specific.
Case report
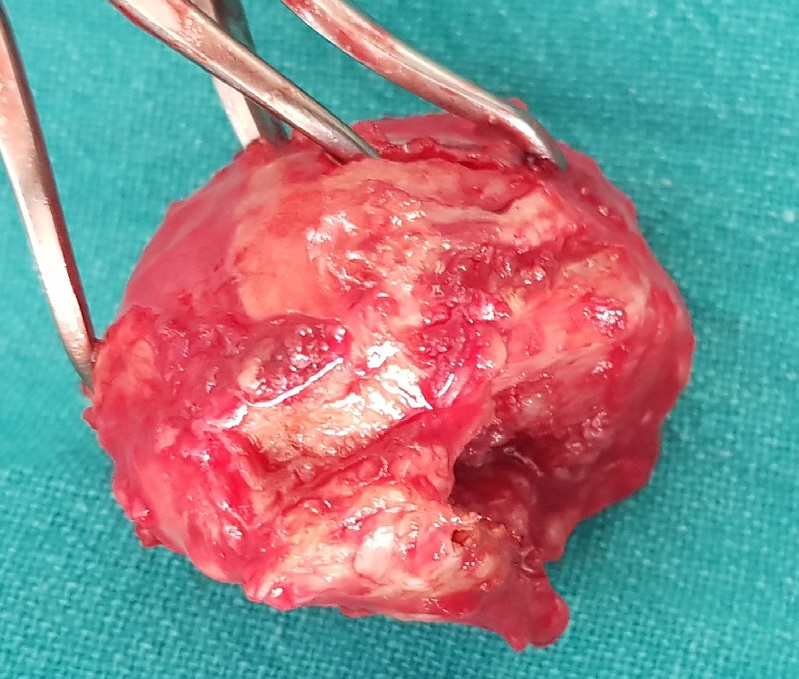
A 43-year old man presented to our department with persistent pain in the left thigh and hip region since almost two years. He complained of marked inability to do activities of daily living without pain and support since around three months. Around 20 years ago, he had undergone management of a para-isthmic femoral shaft fracture sustained in a motorcycle accident with K-nail fixation. Examination revealed painful flexion and external rotation of the left hip. Gait was antalgic and there were markedly painful and restricted activities of squatting and cross-leg sitting. There was occasional tingling along the left lower limb though the distal pulsations were felt adequately. The markers for inflammation or infection including C-reactive protein, total white cell count, erythrocyte sedimentation rate was within normal ranges. The alkaline phosphatase was high. Radiograph of left hip with femur, revealed a oval shaped hypertrophic overgrowth at the tip of a Küntscher nail (K-nail) with smooth contour (Figure 1). It was graded as Brooker grade II HO [9]. Surgical management was done by removal of the callous cap by blunt dissection along the cap with a standard postero-lateral approach to the left hip region in the right lateral posture (Figure 2). The excised cap was hard in consistency with smooth contours and no irregularity (Figure 3). The K-nail was removed by the routine hook engagement extractor instrumentation placed at the eye of the K-nail. The rotation of hip was checked intraoperatively to judge any persisting impingement. Postoperatively, the patient was free of hip pain. Full weight bearing was allowed in the immediate post-operative period. Indomethacin was used prophylactically for an initial two-weeks period. Biopsy confirmed the presence of mature lamellar cortico-spongiosa bone. The two-year follow up showed no recurrence of HO and there was pain-free full weight bearing ambulation with comfortable squatting (Figure 4), active straight leg raising (Figure 5) and cross-leg sitting (Figure 6). An informed consent was obtained from the patient for the use of data for publication.





Discussion
Femoral shaft fractures are normally fixed by IMN as the gold standard treatment [1,10]. The initial fixation device was a K nail. Interlocking nail have been developed subsequently and it gives excellent results in the majority of cases. The K nail have been in use in developing countries as an economical option for isthmic and para-isthmic femoral shaft fracture management [1,11,12]. However, K nail has also been used for the management of compound fractures, polytrauma, irreducible or vascular injured femoral shaft fractures [11]. The K- nail has been advocated in developing countries because of its low cost, ease of insertion, short duration of surgery, poor availability of IMN instrumentation and steep technical learning curve for the use of IMN [10,12]. Common complications associated with femoral nailing includes fat embolism, thermal necrosis, neurovascular injury, iatrogenic fractures (femoral neck, trochanter or femoral condylar fractures), delayed union, nonunion or malalignment [1,13]. An uncommon and infrequently reported complication of IMN or K nail has been the acquired form of HO though few studies report an incidence as high as 68% [1,14]. A late presenting HO with delayed symptomatology is rarely discussed.
HO is the formation of heterotopic bone in soft tissues where it is normally non-existent [15]. Acquired form of HO can also occur with head injury, polytrauma, high injury severity score, hip arthroplasty, acetabular fracture surgery, burns and spine injury with paraplegia [1-3,5,8,14,16]. Hip region may be affected commonly followed by elbow and knee region [1,5]. They have been infrequently reported in paediatric age group along titanium K-wires and TENS nail [2]. Floating knee injuries may present patellar tendon HO more commonly following a combined tibial and retrograde femoral nailing, though the knee function was reported to be preserved without any significant compromise [3].
The HO needs to be differentiated from metastatic calcification which occurs with hypercalcemia and dystrophic calcification associated with tumour [15]. Bone scanning may be required to rule out bone forming tumour osteosarcoma or osteochondroma. The smooth contour of HO in our case presumably, had benign pathological nature.
There have been various reasons attributed to the etiopathogenesis and formation of heterotrophic bone at the nail entry point. However, no definitive reason is known though local and systemic influences have been considered for its causation [1,4,14,16]. The entry point through the proximal femoral end has been either from the piriformis fossa or the tip of greater trochanter. The sharp instrument used for making an entry point and the subsequent reaming of the tract may damage the muscular structures along the tract namely short external rotators, gluteus medius and piriformis producing haematoma and osteoprogenitor cell proliferation [5,6,14,16]. Cadaveric study for entry-point soft tissue damage in antegrade femoral nailing concluded that piriformis fossa entry point has significant muscle damage and trochanteric tip entry point biomechanically facilitated a smoother nail introduction [17]. The protrusion of the proximal nail-end may also irritate the soft tissue envelope and cause repetitive muscle trauma to induce ectopic bone formation [2,6]. This theory though, was refuted in the study on etiopathogenesis factors for HO in IMN cases [5]. Bone morphogenetic protein and prostaglandin E2 have been postulated to cause differentiation of mesenchymal cells to osteoprogenitor cells [15]. The inactivity following any injury, surgery or implied rest or immobilisation followed by mobilization and exercises are common feature leading to formation of HO [8]. A reamed nail had more chances for formation of HO as compared to a non-reamed nail [1,14]. However, reaming debris being a causative factor for HO has not been clearly established [1,16].
Majority of HO require no active treatment as it remains asymptomatic without any functional impairment [1,5,16]. HO may be incidentally identified on radiographic evaluation and may be suggested for “supervised neglect”. The HO may occasionally progress to cause compression or pressure symptoms with painful restricted joint movements. Pressure ulcers, peripheral nerve entrapment and hip ankylosis features may complicate HO and may lead to delayed symptomatology [15]. The symptomatic callus cap requires management. The options in literature include irradiation, steroids, non-steroidal anti-inflammatory drugs (indomethacin or ibuprofen) or surgical excision [1,5,16].
Surgical intervention for removal of HO with IMN may present unique challenges. The common indication for removal of HO are limited range of joint movements affecting activities of daily routine [8,16,18]. Excision should preferably be planned before joint gets ankylosed. The resection of hip HO for Brooker Grade III or IV have high chances of neurovascular injury to femoral artery and sciatic nerve with reported incidence of iatrogenic fracture neck femur following perioperative hip mobilization [8,9,18]. The timing of resection has been a matter of debate with no clear guidelines to base the criteria for surgical excision [8]. However, HO should be resected when mature to reduce the complications related to haemorrhage and post-operative recurrence [1].
In our case, the presentation of late symptomatology with local compressive signs and restricted hip movements was managed surgically to avoid any further progression to ankylosis or malignant transformation.
Conclusion
K-nail is an infrequently used fixation device now-a-days. An old implanted K-nail may present rarely with a callus cap. The symptomatic acquired HO is even rare. Excision should be considered to preserve the hip joint function and to maintain the ability to do activities of daily living. The report highlights the need to be aware of the uncommon complication associated with an uncommon fixation device and need to revisit the complications with K-nail usage in modern trauma management.
Declarations
Ethic approval: Not considered for a retrospective case report.
Consent for publication: The patient was informed that data from the case would be submitted for publication and patient gave the consent.
Acknowledgements: None to declare.
Conflicts of interest: None to declare.
References
- Kow RY, Low CL, Jaya Raj J, VA Jacob A, ESK Mor Japar Khan. Heterotopic Ossification of the Hip Post Reamed Intramedullary Femoral Nail: A Case Report. Ortho Res Online J. 2019; 5. OPROJ.000619.
- Meyer H L, Burggraf M, Polan C, Husen M, Dudda M, Kauther M D. Lollipop Sign - Ossification at Wire Ends after Osteosynthesis. Journal of Orthopaedic Case Reports. 2019; 9: 52-55.
- Kent WT, Shelton TJ, Eastman J. Heterotopic ossification around the knee after tibial nailing and ipsilateral antegrade and retrograde femoral nailing in the treatment of floating knee injuries. Int Orthop. 2018; 42: 1379-1385.
- Botolin S, Mauffrey C, Hammerberg EM, et al. Heterotopic ossification in the reaming tract of a percutaneous antegrade femoral nail: A case report. J Med Case Reports. 2013; 7: 90.
- Marks PH, Paley D, Kellam JF. Heterotopic ossification around the hip with intramedullary nailing of the femur. J Trauma. 1988; 28: 1207-13.
- Dharmshaktu, Ganesh. Letter to Editor: ‘Callus caps’- an intriguing foot-prints of intramedullary nails. American Journal of Diagnostic Imaging. 2018; 4: 22-23.
- Ivan Marintschev, Sascha Rausch, Albert Fujak, Kajetan Klos, Gunther O. Hofmann & Florian Gras Removal of a femoral nail with osseous overgrowth at the end-cap: A navigated and cannulated minimally invasive technique, Computer Aided Surgery. 2013; 18: 1-2, 41-46.
- Macheras GA, Lepetsos P, Leonidou A, Anastasopoulos PP, Galanakos SP, Tsiridis E. Results from the surgical resection of severe heterotopic ossification of the hip: A case series of 26 patients. Eur J Orthop Surg Traumatol. 2017; 27: 1097-1102.
- Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr. Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am. 1973; 55: 1629– 1632.
- Bharti A, Kumar S, Kushwaha S, et al. Kuntscher Nail: A Forgotten Entity Yet a Reliable Modality in Treatment of Winquist Type I and II Closed Femoral Shaft Fractures. Cureus. 2020; 12: e10608.
- Bajwa Ali, Schnaid E, Sweet MEB. Current indications for open Kuntscher nailing of femoral shaft fractures. East and Central African Journal of Surgery. (ISSN: 1024-297X) 2000; 5.
- A Olasinde. Open Kuntscher Nailing Of Closed Femoral Shaft Fractures: Revisited. The Internet Journal of Third World Medicine. 2005; 3.
- Ioannis V Papachristos. “Complications of Femoral Intramedullary Nailing: What should the Surgeon Remember?”. EC Orthopaedics. 2019; 10: 477-482.
- Furlong AJ, Giannoudis PV, Smith RM. Heterotopic ossification: A comparison between reamed and unreamed femoral nailing. Injury. 1997; 28: 9-14.
- Shehab D, Elgazzar AH, Collier BD. Heterotopic ossification. J Nucl Med. 2002; 43: 346-353.
- Barfield WR, Holmes RE, Hartsock LA. Heterotopic Ossification in Trauma. Orthopedic Clinics of North America. 2017; 48: 35–46.
- Dora, Claudio & Leunig, Michael & Beck, Martin & Rothenfluh D & Ganz R. Entry Point Soft Tissue Damage in Antegrade Femoral Nailing: A Cadaver Study. Journal of orthopaedic trauma. 2001; 15: 488-493.
- Juengteerapanich S, Udomkiat P, Mahaisavariya B. Heterotopic ossification after closed femoral nailing. J Med Assoc Thai. 2012; 95: S99-S103.