
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Carotid angioplasty and stenting-Device related complication: Embolic protection filter-wire retention
Arunmozhimaran Elavarasi1*; Sunil K Narayan2; K Nagarajan3
1 Department of Neurology, All India Institute of Medical Sciences, New Delhi, India.
2 Department of Neurology, Jawaharlal Institute of Postgraduate Medical Education and Research, India.
3 Department of Radiodiagnosis, Jawaharlal Institute of Postgraduate Medical Education and Research, India.
*Corresponding Author: Arunmozhimaran Elavarasi
Department of Neurology, All India Institute of Medical
Sciences, New Delhi, India.
Email: arun_ela@yahoo.com
Received : Nov 22, 2021
Accepted : Jan 06, 2022
Published : Jan 13, 2022
Archived : www.jcimcr.org
Copyright : © Elavarasi A (2022).
Abstract
Carotid stenting with the use of an embolic protection device has become a common procedure done routinely for carotid stenosis. The procedure is usually done in patients with transient ischemic attacks or minor strokes for preventing further strokes. Since it is done on patients who are asymptomatic or minimally symptomatic, the occurrence of complications should be kept as close to nil. It is important to know potential complications to be careful when we subject patients to such interventions which can be rewarding if they go well but can be devastating if things go wrong. Here we present a case of carotid stenosis who underwent successful stenting however had a retained filter wire of the embolic protection device. The patient was managed conservatively and the need for a major surgical procedure to remove the retained device could be avoided.
Citation: Elavarasi A, Narayan SK, Nagarajan K. Carotid angioplasty and stenting-device related complication: Embolic protection filter-wire retention. J Clin Images Med Case Rep. 2022; 3(1): 1555.
Introduction
Carotid stenting with the use of an embolic protection device has become a common procedure done routinely for carotid stenosis. The procedure is usually done in patients with transient ischemic attacks or minor strokes for preventing further strokes. Since it is done on patients who are asymptomatic or minimally symptomatic, the occurrence of complications should be kept as close to nil.
Case presentation
We had a 75-year old gentleman with a 10-year history of well-controlled diabetes and hypertension with sudden onset painless vision loss in his right eye (Figure 1). There were no other deficits. Over the next few days, there was a marginal improvement in his visual acuity.
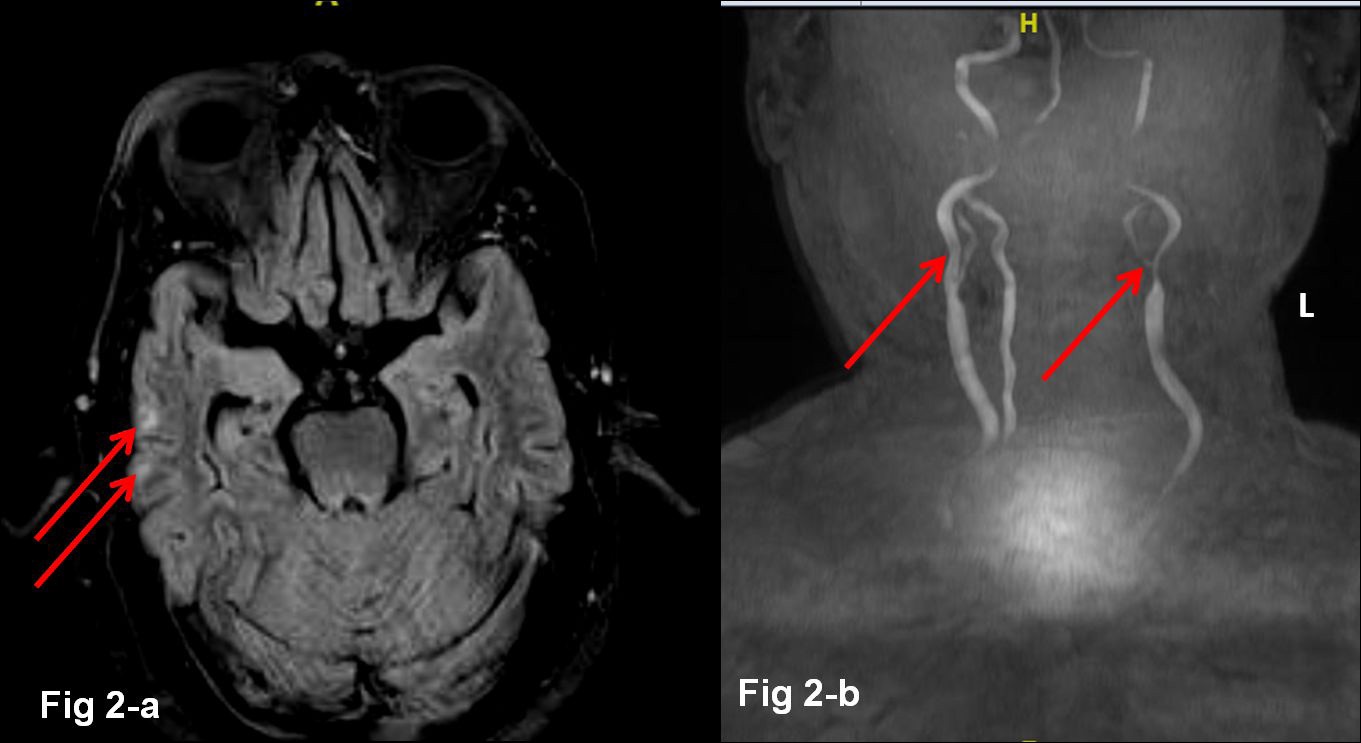
He underwent Magnetic Resonance Imaging (MRI) of the brain which showed age-related mild diffuse atrophy with few white matter T2/FLAIR hyperintense foci (Figure 2a). Computed Tomography (CT) showed calcified plaques in bilateral carotid bifurcation which was more on the right side. CT angiography showed left Internal Carotid Artery (ICA) origin stenosis of 75- 80%.

Procedure note
Digital Subtraction Angiography (DSA) was planned to assess the stenosis and if possible, to do angioplasty and stenting and showed a near-normal right ICA with significant stenosis of the left ICA (70%) (Figure 3). Since the stenosis on the right was not significant and the left was significant, even though it was asymptomatic, it was planned for revascularization. During the right vertebral artery injection, the patient developed sudden restlessness and dysarthria probably related to procedurerelated emboliform showers to the posterior circulation.
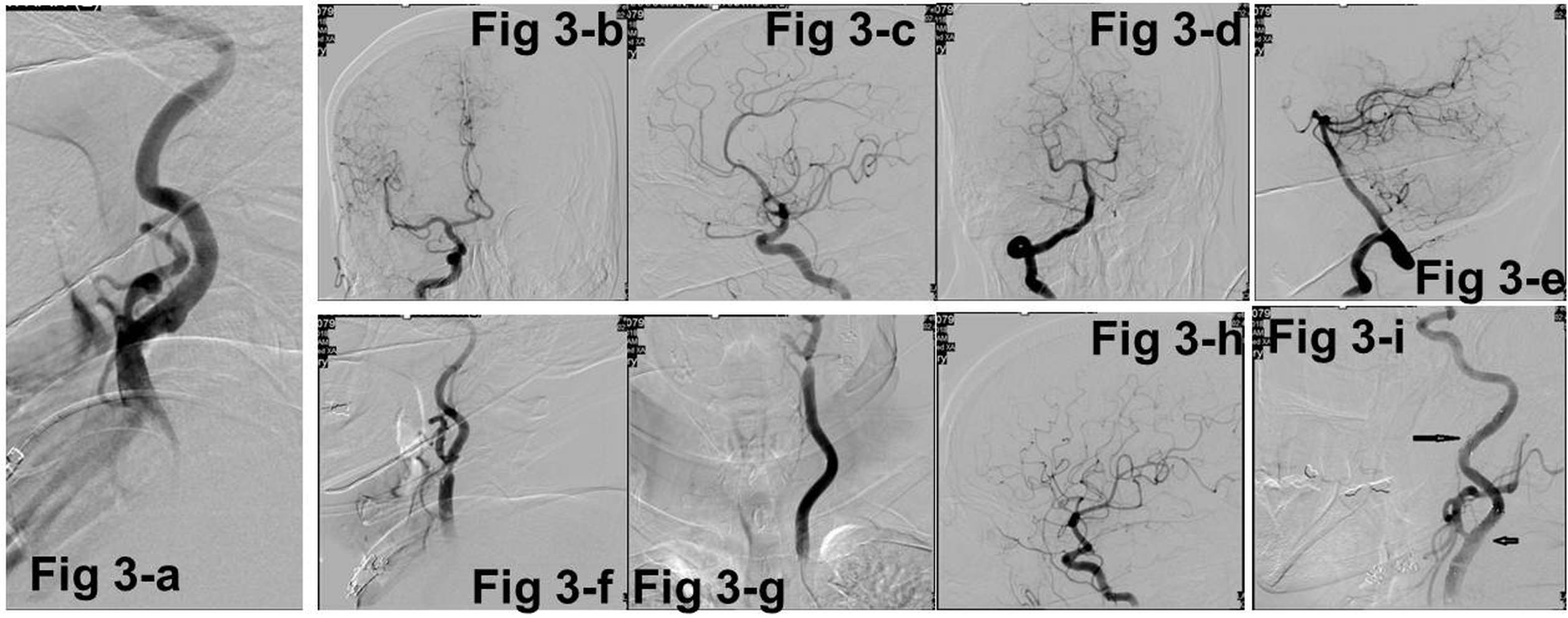
Stenting: The diagnostic catheter was exchanged for a long (90 cm) 7F sheath through stiff Teflon exchange wire placed in the left proximal CCA. The long sheath was placed in the left proximal CCA and 014 filter wire was used to deploy Spider filter (6 mm) in petrous ICA after crossing the stenosis. The stenosis was dilated using a coronary balloon (6 x 20 mm). After balloon dilatation, the stent could not be deployed in the monorail filter wire probably due to device malfunction. As balloon dilatation was already done with embolic risk, another 014 wire was used to deploy the stent (Protégé 6 x 30 mm) with the filter wire caught in between the vessel wall and the stent. The stenosis fully opened up without any need for post-stenting dilatation. An attempt was made to pass the retrieval catheter of the filter along the side of the stent but was not successful. As the patient was already on dual anti-platelets (aspirin and ticagrelor), the filter was left in situ and filter wire was cut at the groin. In the immediate post-procedure period, clinical examination showed right ataxic hemiparesis and dysarthria.
Management of the complication
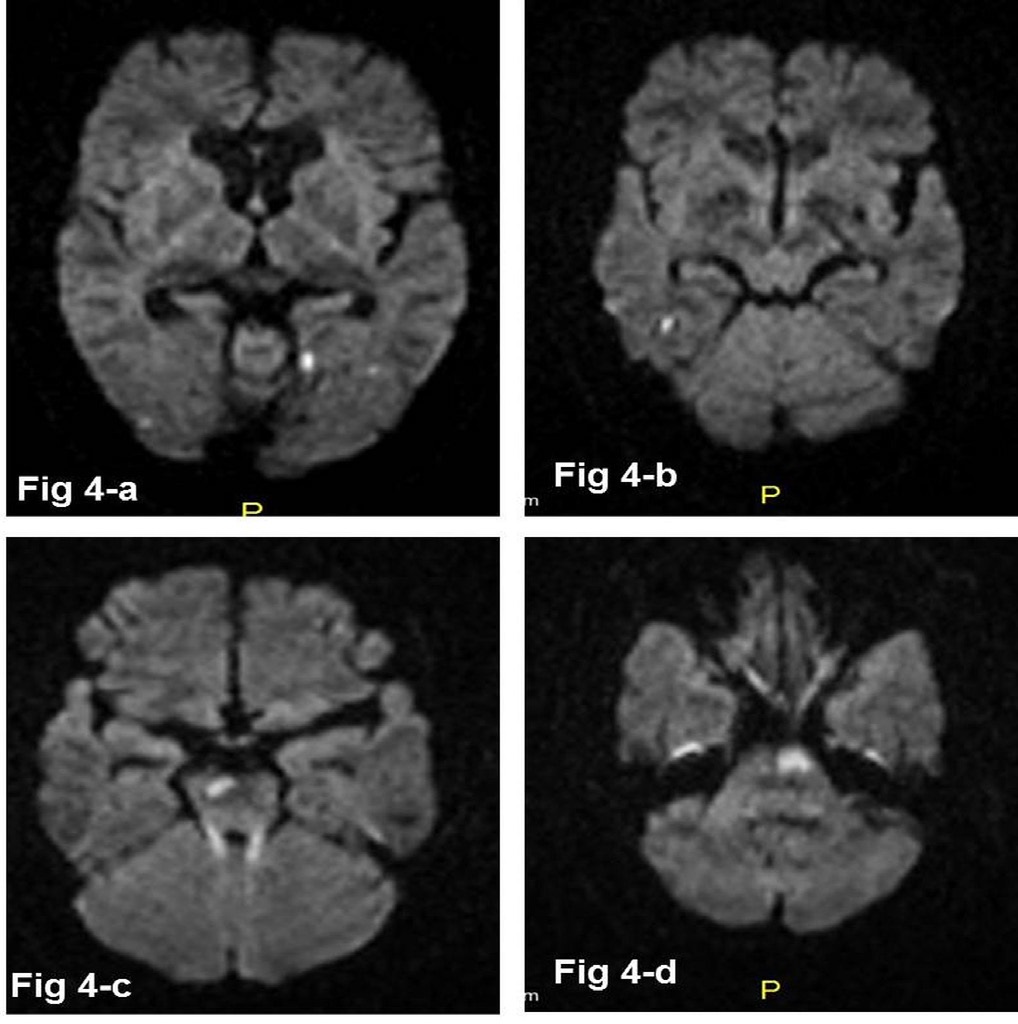
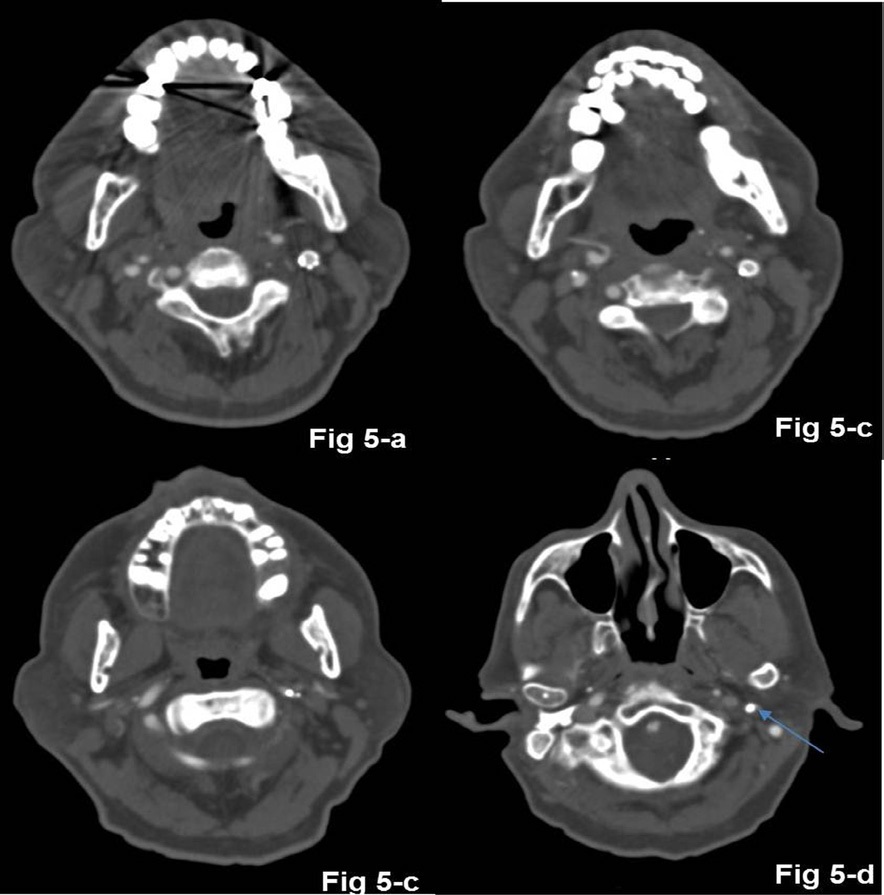
The patient was started on low molecular weight heparin with dual anti-platelets and the patient did not have further deterioration. CT angiography showed the stent and filter device in situ. MRI of the brain revealed multiple small infarcts in the vertebrobasilar circulation probably as emboliform shower (Figure 4). Since he had vascular occlusion in various vascular territories, cardioembolic etiology was strongly considered and echocardiography and 24-hour Holter monitoring was repeated but did not reveal any cardiac source. So patient was kept on triple therapy for a week following which he was discharged on dual antiplatelets. There were no new deficits. He recovered from the hemiparesis by the 4th postoperative week. Follow-up CT angiography (Figure 5) after four-and-half months showed partial non-enhancement in the filter within the distal cervical ICA suggesting partial thrombosis and reduced caliber of left petro-cavernous ICA. There were no infarcts. MRI done after nine months showed no fresh ischemic lesions and stent-filter artifact in left distal cervical and petrous ICA. The left ACA and MCA were seen normally partly due to good cross-flow from opposite right ICA.
Discussion
Imaging features of HCC on MRI
One of the important concerns regarding carotid artery stenting in asymptomatic stenosis is the risk of periprocedural stroke, especially when treating asymptomatic carotid stenosis as stroke can be devastating since the patient is completely asymptomatic, to begin with. With the introduction of embolic protection devices, the periprocedural complication of embolic stroke has been greatly reduced [1], however randomized control trials showed results that were contrary to these reports [2]. Embolic Protection Devices (EPD) are not all that safe and have their complications. In a series of 442 cases who underwent carotid artery stenting with EPD, 0.9% had device-related complications [3]. Malfunction of the device can lead to difficulty in the deployment of the stent as well as an inability to remove the filter leading to device retention [4,5].
In the previous reports of retained EPDs, surgical removal of the device was carried out. Surgical removal of the EPD may be associated with complications such as perioperative stroke or myocardial infarction. The surgical technique of removing the device also necessitated the removal of the stent as well followed by a carotid endarterectomy in this case. This procedure could add to the morbidity due to the more invasive nature as well as the risk of local hematoma and vascular complications as the patient was on anticoagulation as well as dual antiplatelets. So the patient was decided to be managed with close follow-up in the short term. Since there were no short-term embolic complications, it was decided to observe the patient with annual vascular imaging and plan for surgical removal in case the device develops thrombosis with embolization, which is a reasonable alternative to immediate surgical removal.
Conclusion
It is important to know the potential complications of carotid stenting, as the procedure can be rewarding if they go well, but can be devastating if things go wrong. Conservative management with antiplatelets and anticoagulation may be an alternative to surgical removal of the embolic protection device. Close monitoring of clinical and radiologic parameters to detect stent thrombosis is essential, as the embolic protection device may act as a nidus for thrombosis.
Declarations
Patient consent: Obtained
Ethics approval: Not required for individual case reports.
Author Roles
• Arunmozhimaran Elavarasi was involved in patient selection for the procedure, management of pre and post procedure duration and in drafting the manuscript • Sunil K Narayan was involved in patient selection for the procedure, management of pre and post procedure duration and in reviewing the manuscript • K Nagarajan was involved in interpreting imaging, performing the procedure and drafting the manuscript
References
- Knappich C, Kuehnl A, Tsantilas P, et al. The Use of Embolic Protection Devices Is Associated With a Lower Stroke and Death Rate After Carotid Stenting. JACC Cardiovasc Interv. 2017; 10: 1257-1265.
- Macdonald S, Evans DH, Griffiths PD, et al. Filter-Protected versus Unprotected Carotid Artery Stenting: A Randomised Trial. Cerebrovasc Dis. 2010; 29: 282-289.
- Cremonesi A, Manetti R, Setacci F, Setacci C, Castriota F. Protected carotid stenting: Clinical advantages and complications of embolic protection devices in 442 consecutive patients. Stroke. 2003; 34: 1936-1941.
- Li T, Zha Y, Bo L, Wirthlin DJ, Zhang Q. Surgical management for retained distal embolic protection device and fractured guidewire after carotid artery stenting. J Surg Case Rep. 2016; 2016.
- Page P, Niemann D, Son C, Li Y. Retained distal protection device during carotid artery stenting necessitating carotid endarterectomy: A complication and management considerations. Surg Neurol Int. 2018; 9.