
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Rare case of COVID-19 pneumonia in a neonate
Omotakin Omolokun*; Hiba Elhassan
Paediatrics Department, Prince Charles Hospital, Cwm Taf University Hospital Health Board, Merthyr Tydfil, United Kingdom.
*Corresponding Author: Omotakin Omolokun
Paediatrics Department, Prince Charles Hospital,
Cwm Taf University Hospital Health Board, Merthyr
Tydfil, CF479 DT, United Kingdom.
Email: omotakin@netscape.net
Received : Nov 12, 2021
Accepted : Jan 06, 2022
Published : Jan 13, 2022
Archived : www.jcimcr.org
Copyright : © Omolokun O (2022).
Citation: Omolokun O, Elhassan H. Rare case of COVID-19 pneumonia in a neonate. J Clin Images Med Case Rep. 2022; 3(1): 1557.
Background
Children infected with COVID-19 are often asymptomatic or with very mild symptoms [1]. While the risk of vertical transmission has not been fully elucidated [2], it is less common for newborns to have serious infection. We report a case of a 9-day old with COVID-19 Pneumonia requiring mechanical respiratory support.
Case report
A 9 day old baby presented to ED with a three day history of lethargy, and a one-day history of chesty cough, recessions and poor feeding.
He was born by spontaneous delivery at 40 weeks, with a birth weight of 2.9 kg. He had been observed for 12 hours on account of a meconium stained liquor. He was discharged home asymptomatic and bottle feeding. His mother had tested positive for COVID-19 on the day of delivery from routine screening, but was asymptomatic.
On return to the hospital, he examined well with no chest signs. His oxygen saturation was 95% on air and respiratory rate was normal at 46/minute. Mother gave additional history that father had been positive for COVID -19 two days after baby had come home from hospital. (His sibling also tested positive).
We admitted him for observation and for monitoring of milk intake. Nasopharyngeal swabs sent was negative for extended respiratory panel but positive for SARS CoV-2.
Following a feed on day 1 of admission, he developed increased work of breathing with low saturations to 85%.
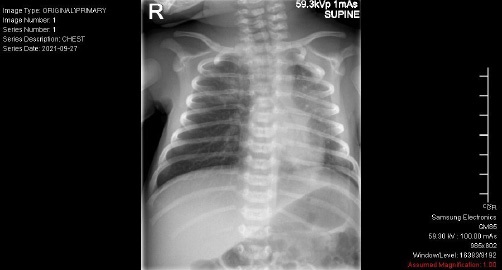
In spite of nasal cannula oxygen of up to 2 litres, he continued to show signs of respiratory distress; tracheal tug, intercostal recessions and low oxygen saturations. He was screened for possible sepsis with blood work and a chest x-ray. His feeds were stopped, he was started on 8 L/min of high flow in Fio2 of 37% to maintain good level of oxygen saturations, and he was started on some IV fluids and antibiotics.
X-rays returned to show patchy alveolar infiltrates throughout the lungs particularly in the right upper zone (See below Figure).
While being monitored, he developed multiple episodes of apnoeas, with some requiring stimulations. There were added concerns about bradycardias and worsening blood gases, so he was switched to nasal CPAP on pressures of 7 cm of water, in Fio2 of 35%.
He was reviewed by the anaesthetic team and was discussed with the regional transport team for the potential of a PICU transfer.
Following advice, he received a loading dose of IV caffeine citrate.
An extended respiratory panel was repeated on day 3 for the chance there was a concurrent respiratory virus responsible for his severe symptoms but results had returned exactly the same as previous result.
On CPAP he gradually started showing some improvement and slowly got better and was weaned to High flow, low flow and air. He completed a five days of antibiotics with a maximum CRP of 84 mg/L and negative blood culture. He was discharged home on day 6 of admission with a plan for outpatient follow up.
Discussion
Transmission
Our baby developed symptoms on the day 6 of life and more than likely infection was from a vertical transmission rather than acquired. While recommendations for COVID positive mothers vary from country to country, [3] our current practice is to advise on strict hand hygiene measures, with wearing of face mask before contacts and preferably for mothers to breastfeed [4]. Asymptomatic mothers are generally NOT separated from their babies. While these measures while could suffice for prevention of acquired cases, it would be considered too late for babies with intrapartum exposure.
Our case is contrary to finding from the New York study where of the 82 babies tested from the 116 COVID positive mothers, none was shown to have the virus [5].
Testing
Our current stance is not to perform COVID testing on newborn with positive mothers unless they develop symptoms or need special baby unit admission. All newborns to COVID positive mothers are offered a baby follow up in 6 weeks
Symptoms
Of note in our baby was the absence of documented fever throughout his 6/7 days in hospital. He was hypothermic on admission with a temperature of 35.6o C but was normothermic for the rest of his stay. We had similarity with the case report by Needleman JS et al on the 3 week old with recurrent apnoea secondary to COVID-19 [6]. Our baby development recurrent episodes of apnoeas many requiring assistance. As this was not a familiar finding in COVID-19 we repeated our extended respiratory panel to exclude other viruses and excluded neonatal sepsis, however we had negative results.
Treatment
Very few of the clinical trials that led to approval of medication for treatment of COVID-19 involved children, [7-9] and never so in neonates. As severe cases in the age group are rare, it would be difficult to conduct randomised placebo control trial to prove efficacy. Dexamethasone is a drug that is available for use in our age group for other reasons. With COVID-19, current recommendation (in older children) is for consultation with a Paediatric Infectious disease specialist on its use for severe case [7]. It will be interesting to find out other clinicians experiences in its use in the context of COVID-19 in newborn.
Vaccinations
Pregnant women are at increased risk of developing severe disease compared with non-pregnant women of the same age. [10].
We take solace in the knowledge that current recommendation is that pregnant women are offered the COVID vaccines. [10].
Conclusion
Serious infection from COVID-19 in the newborn is rare, and as we continue to learn about this evolving disease, a preventative approach is more beneficial than a treatment option. Vaccination remains the best way pregnant women can protect themselves and their babies.
References
- Morand A, Fabre A, Minodier P, et al. COVID-19 virus and children: What do we know? Arch Pediatr. 2020; 27: 117 –118.
- Lopes de Sousa ÁF, et al. Effects of COVID-19 infection during pregnancy and neonatal prognosis: What is the evidence? Int. J. Environ. Res. Public Health 17, E4176. 2020.
- Lavizzari A, Klingenberg C, Profit J, Zupancic JAF, Davis AS, Mosca F, et al. International comparison of guidelines for managing neonates at the early phase of the SARS-CoV-2 pandemic. Pediatr Res. 2020; 89: 940–951. https://doi.org/10.1038/s41390-020- 0976-5
- Royal College of Obstetricians & Gynaecologists. National guidance on managing coronavirus infection in pregnancy published. Royal College of Obstetricians & Gynaecologists. 2020.
- Salvatore CM, Han JY, Acker KP, Tiwari P, Jin J, et al. Neonatal management and outcomes during the COVID-19 pandemic: An observation cohort study. Lancet Child Adolesc Health. 2020; 4: 721-727.
- Needleman JS, Hanson AE. COVID-19-associated apnea and circumoral cyanosis in a 3-week-old. BMC Pediatr. 2020; 20: 382.
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available at https://www.covid19treatmentguidelines. nih.gov/. Accessed [11/14/2021].
- Lutz JD, Mathias A, German P, Pikora C, Reddy S, Kirby BJ, et al. Physiologically-Based Pharmacokinetic Modeling of Remdesivir and Its Metabolites to Support Dose Selection for the Treatment of Pediatric Patients With COVID-19. Clin Pharmacol Ther. 2021; 109: 1116-1124.
- (ox.ac.uk, 2020) Dexamethasone reduces death in hospitalised patients with severe respiratory complications of COVID-19. Available at: http://www.ox.ac.uk/news/2020-06-16-dexamethasone-reduces-death-hospitalised-patients-severe-respiratorycomplications (14/11/2021).
- Principi N, Esposito S. Is the Immunization of Pregnant Women against COVID-19 Justified? Vaccines (Basel). 2021; 9: 970.