
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Biventricular thrombi in a patient with methamphetamine induced dilated cardiomyopathy
Ibiyemi Oke*; Smit Shah; Chris Reggio; Riju Gupta; Rajesh Reddy
Department of Medicine, Reading Hospital, Tower Health System, West Reading, Pennsylvania, USA.
*Corresponding Author: Ibiyemi Oke
Department of Medicine, Tower Health System, Reading
Hospital, 301 S 7th Avenue, West Reading, PA, 19611,
USA.
Email: Ibiyemi.oke@towerhealth.org
Received : Oct 28, 2021
Accepted : Jan 07, 2022
Published : Jan 14, 2022
Archived : www.jcimcr.org
Copyright : © Oke I (2022).
Citation: Oke I, Shah S, Reggio C, Gupta R, Reddy R. Biventricular thrombi in a patient with methamphetamine induced dilated cardiomyopathy. J Clin Images Med Case Rep. 2022; 3(1): 1564.
Case description
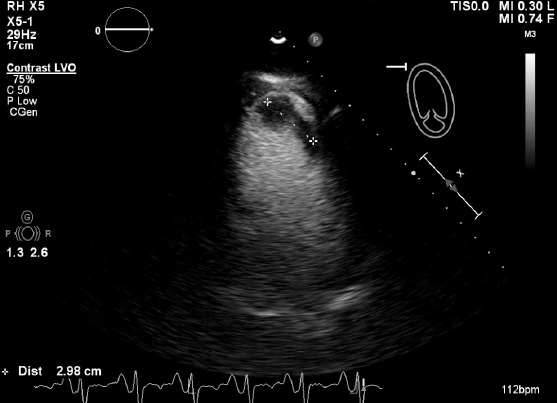
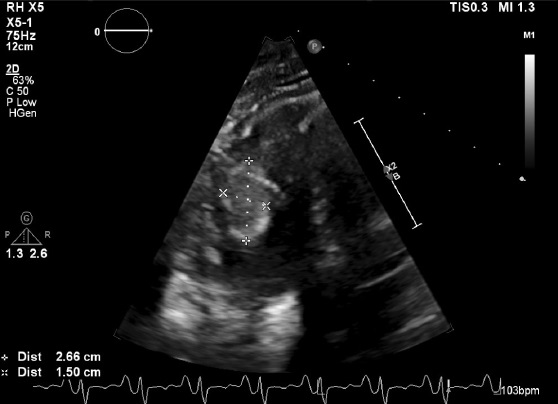
A 39-year-old male with a 20-year history of cannabis and methamphetamine abuse presented to the ER with progressive shortness of breath, orthopnea, and bilateral leg swelling.Temperature 36.8°C, pulse 116/min, blood pressure 125/89 mmHg, respiratory rate 18/min, oxygen saturation 93% on room air. He had 2+ bilateral pitting pedal edema, elevated JVD, and S3. He had elevated BNP and creatinine, low magnesium, and potassium. UDS was positive for Amphetamine and THC (Marijuana) but normal Ethanol level. EKG was sinus rhythm, PVCs, and non-specific T wave changes; CXR showed cardiomegaly with pulmonary vascular congestion. CT chest revealed an indeterminate well-circumscribed filling defect in the right ventricle’s apex concerning for a thrombus versus neoplastic nodule. Transthoracic Echocardiography (TTE) findings of biventricular dilatation, global hypokinesis, right and left apical thrombus, a 5 X 3.2 cm mass in the right ventricle, Left Ventricular Ejection Fraction (LVEF) of 15 to 20%, grade 2 diastolic dysfunction, and Pulmonary Artery Systolic Pressure (PASP) of 40 mmHg (Figure 1a & 1b). He had widely patent coronary arteries on left heart catheterization, but Right heart catheterization showed elevated pulmonary capillary wedge pressure. Thrombophilia screen was negative, and there was no Deep Venous Thrombus (DVT) on lower extremity venous Doppler ultrasound.
Methamphetamine (MAA) use may be associated with severely reduced cardiac function and acute heart failure [1]. MAA-induced cardiomyopathy may result from direct myocardial injury and inflammation or indirectly through exaggerated sympathetic drive [2]. Severe systolic dysfunction in these patients may be complicated by cardiac emboli and stroke if not detected early [3]. This patient received intravenous furosemide, and he was discharged on goal-directed medical therapy, Coumadin, and a life vest. He was counseled on abstinence from marijuana and amphetamine and was referred to outpatient addiction medicine.
With the increasing use of methamphetamine, clinicians need to be aware of the potentially devastating complication of cardiomyopathy by embolic stroke.
References
- Singal AK, Deepti S, Sharma G, Kothari SS. Herculean mistake: Mephentermine associated cardiomyopathy. The Physician and sportsmedicine. 2021; 49: 116-122.
- Giv MJ. Exposure to amphetamines leads to development of Amphetamine Type Stimulants Associated Cardiomyopathy (ATSAC). Cardiovascular toxicology. 2017; 17:13- 24.
- Goland S, Luo T, Siegel RJ. Multiple intracardiac thrombi in a patient with dilated cardiomyopathy. Heart. 2006; 92: 1472.