
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Per oral endoscopic myotomy (POEM) in a COVID-19 patient
Shaimaa Elkholy1; Kareem Essam1; Ahmed Ragab El-Gazzarah2; Gina Gamal3; Abeer Awad Abdellatif1*; Mohamed El-Sherbiny1
1 Gastroenterology Division, Internal Medicine Department, Faculty of Medicine, Cairo University, Egypt.
2 Tropical Medicine Department, Faculty of Medicine, Menoufia University, Egypt.
3 Gastroenterology Division, Internal Medicine Department, Faculty of Medicine, Ain shams University, Egypt.
*Corresponding Author: Abeer Awad Abdellatif
Internal Medicine Department, Kasr Al-Aini Hospitals,
Cairo University, Cairo Egypt
Email: beero4a@yahoo.com
Received : Oct 23, 2021
Accepted : Jan 07, 2022
Published : Jan 14, 2022
Archived : www.jcimcr.org
Copyright : © Abdellatif AA (2022).
Abstract
Background: SARS-COV2 pandemic had a great impact on our life. Changes had been done to accommodate the current situation. Infection control measures in the endoscopy units had entirely changed. Also, prioritizations of different procedures had changed especially in the lockdown time. Peroral Endoscopic Myotomy (POEM) is considered a low priority endoscopic procedure.
Case presentation: We report a 12-year-old child complaining of dysphagia and weight loss who was diagnosed as Type II achalasia. She underwent POEM. According to our Egyptian protocol; COVID-19 was excluded pre-procedural. After POEM, immediately post-procedural chest X-ray was done as usual, and it showed a shadow in the right lung base. Accordingly, HRCT of the chest was done and it showed bilateral asymmetrical patchy areas of ground-glass opacities in the posterior segments of both lower lung lobes (CO-RADS 4). PCR for COVID-19 was positive.
Conclusion: We report a very unique COVID-19 case that raises many challengeable issues and shows a useful message about the risk of silent COVID-19 infection in children during the endoscopy.
Keywords: achalasia; Poem; 3rd Space endoscopy; COVID-19.
Citation: Elkholy S, Essam K, Gazzarah ARE, Gamal G, Abdellatif AA, et al. Per oral endoscopic myotomy (POEM) in a COVID-19 patient. J Clin Images Med Case Rep. 2022; 3(1): 1565.
Background
The risk of transmission of Coronavirus-19 (COVID-19) during endoscopy seems to be a challenging issue due to the unavoidable risk of exposure to respiratory secretions and/or feces during the procedure, also asymptomatic COVID-19 infected patients may add another obstacle for infection transmission. A lot of societies exert hugely efforts to minimize this risk through patient triage and risk assessment before endoscopy, resource prioritization, and allocation, regular monitoring of personal protective equipment, infection control measures, protective device training, and implementation of a strategy for a stepwise resumption of endoscopy services after control of the COVID-19 outbreak [1]. Therefore, the benefit of endoscopy should be weighted by the risk of COVID-19 infection to them; therefore prioritizations of different procedures had changed especially in the lockdown time.
According to the European Society of Gastrointestinal Endoscopy (ESGE) position statement, Peroral Endoscopic Myotomy (POEM) is considered a low priority endoscopic procedure [2].
Case presentation
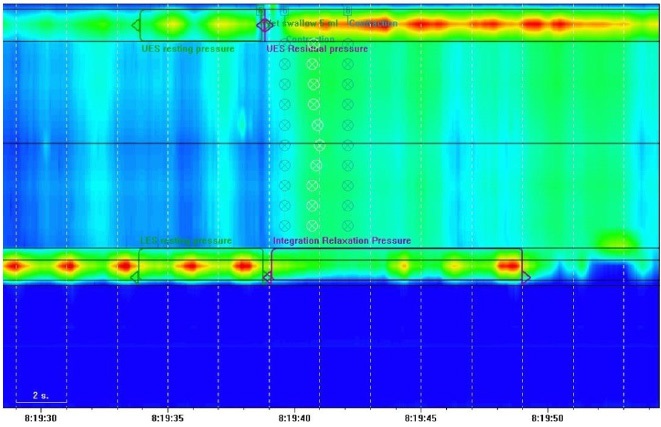
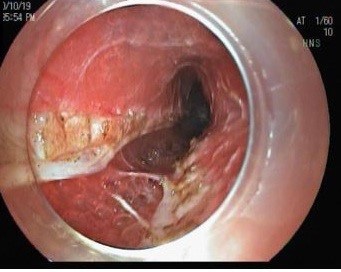
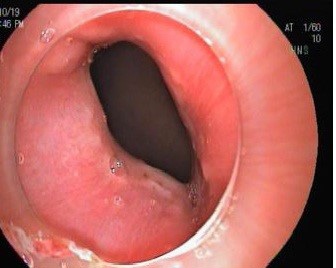
We present a 12-year-old child complaining of dysphagia and weight loss of 10 months duration. Her condition had recently worsened when she started to develop recurrent attacks of vomiting. She was diagnosed to have type II achalasia (Figure 1).
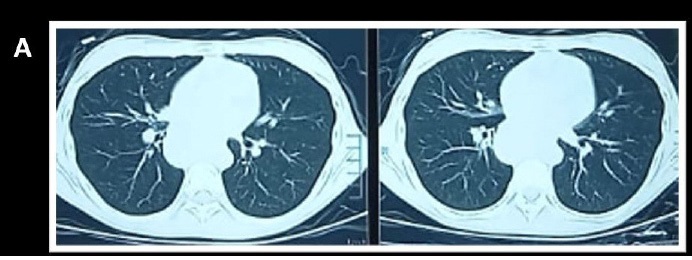
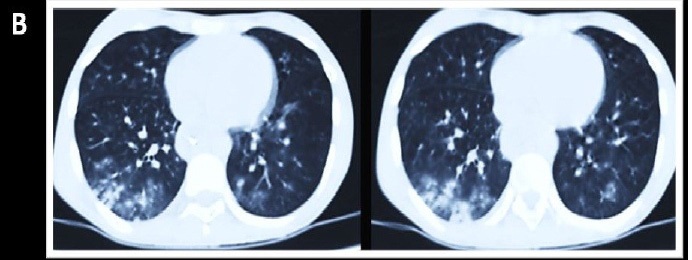
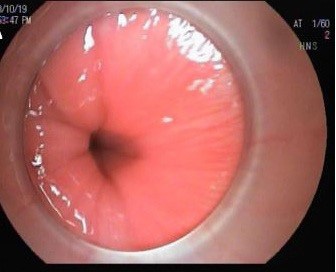
The patient was referred to our center for POEM. According to our hospital’s protocol, prior to admission HRCT scan of the chest, CBC and CRP are routinely done. Our patient had normal results of the HRCT (Figure 2a), CRP was negative, and CBC was normal apart from relative lymphocytosis (2 days before the procedure). The patient had also serological tests for COVID-19; IgG was positive while IgM was negative. The patient was then admitted to our hospital and POEM procedure was done under general anesthesia and mechanical ventilation (Figure 3 shows steps of POEM procedure) [Supplementary Video]. Chest X-ray was done immediately after the procedure as usual; a shadow was seen in the right lung base. HRCT of the chest was done for fear of aspiration pneumonia and the results were shocking. It showed bilateral asymmetrical patchy areas of ground-glass opacities in the posterior segments of both lower lung lobes but more extensive on the right side and scattered fluffy cotton opacities (CO-RADS 4) [Figure 2b]. A Real‐Time Polymerase Chain Reaction (RT-PCR) assay for COVID-19 was done and it was positive. No one from the Health Care Workers (HCW) or her family members who come in close contact develop any symptoms suggestive of COVID-19 infection, however; no screening for COVID-19 infection was done for them.


Discussion
In Egypt, the lockdown had been ended 3 months ago and endoscopic procedures were gradually returned to the usual practice but with different precautions. Currently, despite all precautions that are taken to minimize the risk of COVID-19 transmission during the endoscopy theater; there are still many challengeable issues. Furthermore, asymptomatic COVID-19 infected patients are a recognized source for transmission of infection [3]; the various available data reported that the viral loads detected in asymptomatic patients are similar to those of symptomatic patients, indicating that infection could be transmitted from asymptomatic as similar to symptomatic individuals [4]. Accordingly, the effective prevention and control for apparent infection is early detection and early isolation. Meanwhile, the prevention and control for silent infection is overall isolation and overall disinfection [5].
Some societies recommend testing all patients having an endoscopy of longer than an hour, highlighting the increased risk of infection with prolonged aerosol generation [6].
Based on increasing the risk of coughing and aerosol generation during the long procedures, the risk of endotracheal intubation and mechanical ventilation may be another risk for infection transmission.
In our case and after exclusion of COVID-19 infection according to our national guide [7]; the endoscopic procedure was done, which was followed immediately by typical CT findings of COVID-19 infection.
However, COVID-19 infection seems to be rare and mild in children, with only 2.4% of reported cases occurring in individuals below 19 years old with approximately 2.5% and 0.2% who developed severe and critical illness respectively [8,9]; still, the reason for the lower burden of COVID-19 infection in children is not clear. It could be explained by a lower expression of Angiotensin-Converting Enzyme 2 (ACE2), a receptor for the SARS-CoV-2 spike protein, that increases with age [10]; another explanation may be due to the absence of maladaptive immune responses in children that lead to Acute Respiratory Distress Syndrome (ARDS) as in older age groups [11], however other unidentified mechanisms are still likely.
There are many challengeable questions in our case; the first one is that if the patient developed a subclinical asymptomatic COVID-19 infection that showed negative CT before the procedure then positive CT findings immediately after the procedure or if there is a role for ventilation system in transmission of COVID-19 infection. The available data showed that despite the possibility of COVID-19 spreading through the ventilation system ducts of Heating, Ventilation, and Air-Conditioning (HVAC) systems; there is still no evidence that human infection with SARS-CoV-2 could be caused by infectious aerosols through the HVAC and the risk is rated as very low [12]. The second option, we thought that she might have caught the infection, while she was doing her first HRCT chest as a lot of patients, are doing HRCT chest nowadays and it could be also a possible source of infection.
Another challengeable issue is that despite the usefulness of chest CT for screening for COVD-19 comparable to RT-PCR testing as reported [13]; Our patient showed negative CT chest for COVID pre-procedural that turned immediately to typical CT findings of COVID-19 after the procedure; this could be explained by delayed CT finding than RT-PCR but unfortunately, we could not be sure of that as the patient did not do RT-PCR before the procedure.
Finally, it is challenging to know the exact reason but we believe that this case presents a beneficial message for practice nowadays.
Conclusion
We present here a very unusual case of COVID-19 in an achalasia patientwho underwent a POEM procedure and despite all precautions that were taken; there are still many debatable issues. Silent infection is an obstacle with having an important impact on the risk of infection transmission.
Declarations
Declaration of interest: The authors declare no Conflict of Interests for this article. The authors alone are responsible for the content and writing of the paper.
Funding: Authors received no funding for this study.
No source(s) of support in the form of grants, equipment, drugs.
We confirm that this work is original and has not been published elsewhere, nor it is currently under consideration for publication elsewhere.
We have no financial or other relationships that might lead to a conflict of interest.
The manuscript has been read and approved by all the authors and each author believes that the manuscript represents honest work.
References
- Chiu PWY, Ng SC, Inoue H, et al. Practice of endoscopy during COVID-19 pandemic: position statements of the Asian Pacific Society for Digestive Endoscopy (APSDE-COVID statements). Gut. 2020; 69: 991-996.
- Gralnek IM, Hassan C, Beilenhoff U, et al. ESGE and ESGENA Position Statement on gastrointestinal endoscopy and the COVID-19 pandemic. Endoscopy. 2020; 52: 483.
- Endoscopy activity and COVID-19: BSG and JAG guidance – update 6.04.20. Online. Available from: https://www.bsg.org.uk/ covid-19-advice/endoscopy-activity-and-covid-19-bsg-and-jagguidance/. Accessed the 6th of April, 2020.
- Zou L, Ruan F, Huang M, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020; 382: 1177–1179.
- Geng J, Yu J, Lu T, Wang Y, Cao Y. A Silent Infection Pandemic of COVID-19: Epidemiological Investigation and Hypothetical Models. Can J Infect Dis Med Microbiol. 2020; 2020: 5120253.
- Bhandari P, Subramaniam S, Bourke MJ, et al. Recovery of endoscopy services in the era of COVID-19: Recommendations from an international Delphi consensus. Gut. 2020; 69: 1915- 1924.
- Mostafa, A.S., Abdalbaky, A., Fouda, E.M. et al. Practical approach to COVID-19: an Egyptian pediatric consensus. Egypt Pediatric Association Gaz 68, 28, 2020.
- Brasil. Ministério da Saúde Protocolo de manejoclínico para o novo-coronavírus (2019-nCoV) [2020 Feb 12].
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) [2020 Feb 25].
- Yonker LM, Neilan AM, Bartsch Y, et al. Pediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses. J Pediatr. 2020; 227: 45-52.e5.
- Fialkowski A, Gernez Y, Arya P, Weinacht KG, Kinane TB, Yonker LM, et al. Insight into the pediatric and adult dichotomy of COVID-19: Age-related differences in the immune response to SARS-CoV-2 infection [published online ahead of print, 2020 Jul 25]. Pediatr Pulmonol. 2020; 10.1002/ppul.24981.
- European Centre for Disease Prevention and Control. Heating, ventilation and air-conditioning systems in the context of COVID-19. 10 November 2020. Stockholm: ECDC; 2020.
- Fang Y, Zhang H, Xie J, et al. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology. 2020; 296: E115-E117.