
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Salmonella arteritis as an unusual cause of hydroureteronephrosis: Case report and literature review
Wu Johnny; Srour Maria; Bokhari Amber; Frey Sharon; Abate Getahun*
Saint Louis University, Missouri, USA.
*Corresponding Author: Getahun Abate
Division of Infectious Diseases, Allergy and Immunology, Saint Louis University, USA.
Email: getahun.abate@health.slu.edu
Received : Oct 28, 2021
Accepted : Jan 07, 2022
Published : Jan 14, 2022
Archived : www.jcimcr.org
Copyright : © Abate G (2022).
Abstract
We report a case of internal iliac pseudoaneurysm complicated by hydroureteronephrosis in a newly diabetic 76 year old woman with Salmonella enterica serovar Choleraesuis bacteremia. She was treated with endovascular coiling and levofloxacin and was discharged in stable condition. To our knowledge, this is the first reported instance of Salmonella iliac arteritis complicated by hydroureteronephrosis. The suspicion for Salmonella arteritis should be high when signs of infection are present.
Keywords: salmonella; Iliac artery; arteritis; hydroureteronephrosis; pseudoaneurysm.
Citation: Johnny W, Maria S, Amber B, Sharon F, Getahun A. Salmonella arteritis as an unusual cause of hydroureteronephrosis: Case report and literature review. J Clin Images Med Case Rep. 2022; 3(1): 1568.
Introduction
Arteritis is a dangerous complication of Salmonella infection that usually affects large, atherosclerotic vessels, such as the thoracic and abdominal aorta. If a pseudoaneurysm develops, it may exert a mass effect upon the surrounding tissue and create organ-specific symptoms [1,2]. One example is polyuria, seen in our patient. This was caused by hydroureteronephrosis from the growing pseudoaneurysm and successfully treated by ureteral stenting and then endovascular coiling of the pseudoaneurysm.
Case report
A 76 year old woman with no significant medical history presented to a community hospital with right hip and right pelvic pain. Over the preceding four months, she suffered multiple falls without radiographic fractures as well as subjective fever, chills, night sweats, and polyuria. Over the past year, she had a 30 pound unintentional weight loss. She denied nausea, vomiting, diarrhea, bloody stools, dysuria, or vaginal discharge. In the remote past, she had two right hip arthroplasties for femur fractures without complication and a hysterectomy with bilateral salpingo-oopherectomy. She worked as a grocery store cashier and lived with her adult daughter and two cats. There were no known sick contacts or recent travel.
On admission to an outside hospital, she had a temperature of 102°F and was slightly hypertensive but otherwise hemodynamically stable. She experienced a single episode of oxygen desaturation to 86%. Abdominal exam revealed tenderness in the right lower quadrant and over the right iliac crest without any palpable mass. Her cardiovascular, respiratory, neurological, and skin examinations were normal.
Laboratory findings were notable for a White Blood Cell count (WBC) of 17.45 thousand/mm3 , C-reactive protein of 6.16 mg/ dL, a lactic acid of 14.5 mg/dL, and glycated hemoglobin of 7.3. After blood and urine cultures were drawn, empiric ceftriaxone was started for possible urosepsis. A Computerized Tomography (CT) scan of the chest using pulmonary emboli protocol and CT with contrast of the abdomen and pelvis revealed a right pelvic mass with a 2.7 Centimeter(cm) diameter near the right internal iliac artery with obstructed ureter and hydronephrosis. On the second day of admission, right ureteral stent was placed. On the fourth day of admission, the initial blood cultures grew Salmonella enterica serovar Choleraesuis, and when sensitivities two days later showed resistance to ceftriaxone, she was switched to meropenem. A transthoracic echocardiogram showed no valvular vegetations or dysfunction. A repeat CT with contrast of the abdomen and pelvis on the sixth day was consistent with an interval decrease in the size of the pelvic mass, and an Indium-111 WBC scan showed no active infectious process. On the ninth day of admission, her fever and leukocytosis had resolved, and meropenem was switched to levofloxacin. A third CT abdomen and pelvis on the same day demonstrated a persistent mass. On the thirteenth day of admission, she was transferred to our institution for further workup and management.
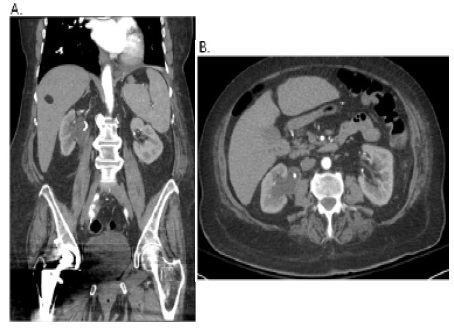
Upon arrival, she was afebrile and hemodynamically stable and complained of continuing right hip and pelvic pain. However, a palpable right pelvic mass was now present on exam. A CT angiography of abdomen and pelvis demonstrated a right proximal internal iliac artery pseudoaneurysm with a diameter of 2.0 cm with possible contained rupture and right hydroureteronephrosis extending to the pseudoaneurysm (Figure 1). Repeat blood cultures were negative, and RPR and HIV test were non-reactive. She was continued on levofloxacin and started on metronidazole. On the seventh day of admission to our hospital, endovascular coil embolization of the pseudoaneurysm was performed without complication. After the procedure, her pelvic pain completely resolved, and the mass could no longer be palpated. Metronidazole was discontinued and patient was discharged on oral levofloxacin to be continued for a total of at least six weeks from the time of endovascular coiling. At her six week follow-up appointment with vascular surgery, she reported continued absence of any right hip and pelvic pain. A repeat CT angiography of her internal iliac artery showed resolution of inflammation and good positioning of the coils.
Discussion
Non-typhoidal Salmonella enterica commonly cause self-limiting gastroenteritis after exposure to contaminated water, food, or animals, with bacteremia occurring in about 5-10% of these cases [1]. Systemic infections, including pneumonia, septic arthritis, endocarditis, and arteritis, occur rarely with bacteremia but almost always in immunocompromised or elderly patients [1]. Unlike many other serovars, Choleraesuis usually causes bacteremia without any preceding gastrointestinal symptoms and has a predilection for causing endovascular disease in atherosclerotic arteries [1,2]. The most commonly affected vessels are the thoracic and abdominal aorta and femoral arteries, and to our knowledge, there have only been a handful of cases involving the internal iliac artery.
Early diagnosis of Salmonella arteritis is challenging but critical to prevent severe hemorrhage or fulminant sepsis. Symptoms are non-specific, with the most common being fever, malaise, and weight loss [2]; a mass is not always palpated, such as in our patient. Furthermore, the mass effect of the aneurysm or pseudoaneurysm can also cause significant comorbidities, clouding the clinical picture. In our patient, the internal iliac pseudoaneurysm compressed the adjacent ureter, causing hydroureteronephrosis that required ureteral stenting. Her resulting polyuria was suggestive of a urinary tract infection rather than arteritis, and the pelvic mass initially seen on CT abdomen and pelvis was interpreted as a possible abscess or malignancy rather than a pseudoaneurysm. Her diagnosis was ultimately narrowed by a positive Salmonella blood culture, which is found in only 50-75% of patients but should prompt immediate imaging. The imaging modality of choice is CT angiography, which has a sensitivity and specificity of 92-96% and 93-100%, respectively [3,4]. Other modalities, such as CT or Indium-111 WBC scans, are not recommended due to inferior sensitivities [3,4].
The traditional treatment of Salmonella arteritis is surgical resection and bypass of the vessel along with long term antibiotics for at least six weeks. In aortitis, this combined approach has a 40% mortality rate compared to a 96% mortality rate with antibiotics alone [2]. More recently, the use of endovascular repair instead of open surgery has gained traction in certain patient populations [5-7]. Since the surrounding tissue cannot be debrided endovascularly, this technique is reserved for patients without sepsis, gross purulence, or infection. While short and medium term outcomes have been equivalent to those from open surgery, long term outcomes have not been well studied [8]. Because there is a theoretical risk of persistent infection following endovascular repair, patients are sometimes placed on lifelong antibiotic therapy.
Of the endovascular surgeries, coil embolization is used infrequently compared to stent-grafting in mycotic aneurysm and pseudoaneurysm repairs. In the literature, this procedure has been used to treat subclavian and splenic pseudoaneurysms, but to our knowledge, this patient is the first to receive it as the sole surgical treatment of a Salmonella infected internal iliac pseudoaneurysm [9,10]. Although her long-term prognosis is still unclear, the proper positioning of the coils and absence of pain after six weeks are suggestive of at least short term efficacy.
Conflicts of interest: The authors have no conflict of interest report and no funding was obtained for the care of the patient included in the case report or preparation of manuscript. The case report does not include patient identifiers and uses data collected in a routine clinical care.
References
- Chiu CH, Su LH, Chu C. Salmonella enterica serotype Choleraesuis: Epidemiology, pathogenesis, clinical disease, and treatment. Clin Microbiol Rev. 2004; 17: 311-322.
- Soravia Dunand VA, Loo VG, Salit IE. Aortitis due to Salmonella: Report of 10 cases and comprehensive review of the literature. Clin Infect Dis. 1999; 29: 862-868.
- Lee WK, Mossop PJ, Little AF, Fitt GJ, Vrazas JI, et al. Infected (mycotic) aneurysms: Spectrum of imaging appearances and management. Radiographics. 2008; 28: 1853-1868.
- M. Fisk LFP, K. Miyagi, M.J. Steward, S.F. Lee, M.B. Macrae, et al. Mycotic aneurysms: A case report, clinical review and novel imaging strategy, QJM: An International Journal of Medicine. 2012; 105: 181-188.
- Cury MV, de Campos MH, Dos Santos DP. Salmonella related mycotic pseudoaneurysm of the superficial femoral artery. Int J Surg Case Rep. 2012; 3: 27-29.
- Sundar G AM, Keshava SN, Boddu D, Chaudhary NK. Mycotic Pulmonary Artery Pseudoaneurysm in a Child Treated by Endovascular Coil Embolization. Vascular Management. 2015; 12: E242- E246.
- Asai M, Van Houtte O, Sullivan TR, Garrido M, Pineda DM, et al. Endovascular Repair of Three Concurrent Mycotic Pseudoaneurysms. Vasc Endovascular Surg. 2018; 52: 473-477.
- Strahm C, Lederer H, Schwarz EI, Bachli EB. Salmonella aortitis treated with endovascular aortic repair: A case report. J Med Case Rep. 2012; 6: 243.
- Tekola BD, Arner DM, Behm BW. Coil migration after transarterial coil embolization of a splenic artery pseudoaneurysm. Case Rep Gastroenterol. 2013; 7: 487-491.
- Chen YF, Su CS, Liu TJ, Chang MS, Jong GP, Ting CT, et al. Endovascular treatment of a nontraumatic left subclavian artery pseudoaneurysm. J Chin Med Assoc. 2012; 75: 474-478.