
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Too close for comfort: A case of extrinsic compression of the left ventricle by a large hiatal hernia
Ibiyemi Oke*; Smit Shah; Christopher Reggio; Riju Gupta; Rajesh Reddy
Department of Medicine, Reading Hospital, Tower Health System, West Reading, Pennsylvania, USA.
*Corresponding Author: Ibiyemi Oke
Department of Medicine, Tower Health System, Reading
Hospital, 301 S 7th Avenue, West Reading, PA, 19611,
USA.
Email: Ibiyemi.oke@towerhealth.org
Received : Oct 28, 2021
Accepted : Jan 10, 2022
Published : Jan 17, 2022
Archived : www.jcimcr.org
Copyright : © Oke I (2022).
Citation: Oke I, Shah S, Reggio C, Gupta R, Reddy R. Too close for comfort: A case of extrinsic compression of the left ventricle by a large hiatal hernia. J Clin Images Med Case Rep. 2022; 3(1): 1569.
Description
A 77-year-old man with a history of Coronary artery disease, COPD, and pulmonary fibrosis on 5 L of oxygen at home presented to the emergency department with dizziness.
Vital signs at presentation included temperature 37°C, pulse 160/min, blood pressure 86/60 mmHg, respiratory rate 24/min, oxygen saturation 96% on 5 L of oxygen. He had end-inspiratory crackles on lung auscultation.
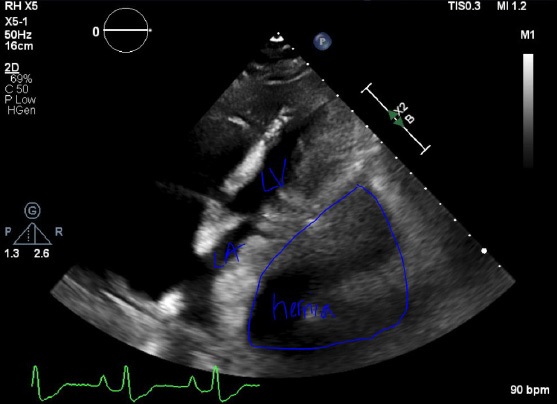
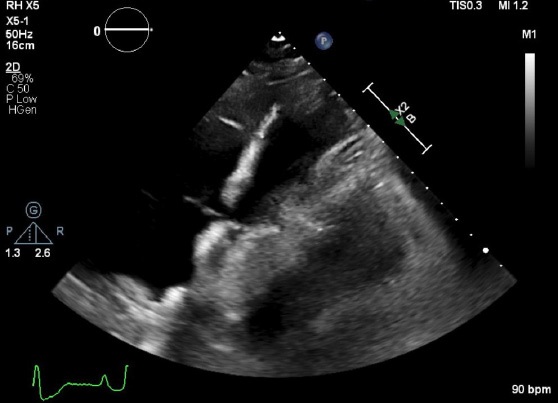
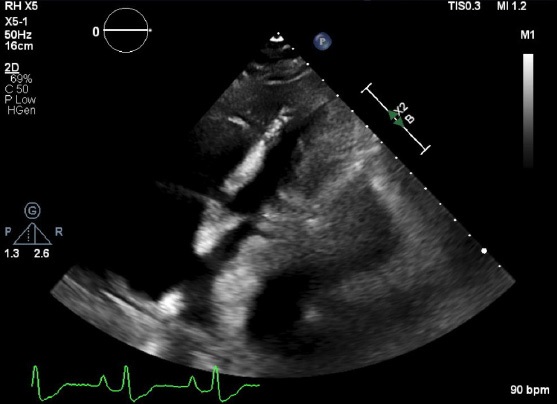
His labs were unremarkable, but he had atrial fibrillation with a ventricular rate of 162 and non-specific T wave changes on EKG. Chest X-ray showed prominent interstitial markings representing fibrosis, and Chest CT revealed a large hiatal hernia with left pleural thickening and worsening emphysema. Transthoracic Echocardiogram (TTE) showed an Ejection fraction of 75%, extrinsic compression of the inferior, lateral, and inferolateral wall, and impaired relaxation. Other Echocardiographic findings were extrinsic compression of the left atrium, dilated right atrium, moderate tricuspid regurgitation, and estimated right ventricular systolic pressure of at least 96 mmHg (Figures 1a,b&c).
Cardiac distortion by a large hiatal hernia can increase the risk of various forms of arrhythmia and Left Ventricular Outflow Obstruction (LVOT), leading to syncope and exertional dyspnoea [1,2]. Although this patient had severe COPD and pulmonary fibrosis, his TTE abnormalities showed that his dyspnea may have been partly due to left atrial and ventricular compression by his large hiatal hernia. Interestingly, this patient only reports intermittent reflux symptoms, and he was not on proton pump inhibitors. The hemodynamic effect on cardiac structures can become accentuated when the hernia increases in size during feeding [3]. Hernia surgery often leads to symptomatic improvement. In this case, the patient was deemed not a surgical candidate due to severe COPD and interstitial fibrosis. His atrial fibrillation was treated, and he was discharged on metoprolol and Apixaban.
References
- Naoum C, Falk GL, Ng AC, Lu T, Ridley L, Ing AJ, Kritharides L, Yiannikas J. Left atrial compression and the mechanism of exercise impairment in patients with a large hiatal hernia. Journal of the American College of Cardiology. 2011; 58: 1624-1634.
- Harada K, Tamura U, Ichimiya C, Terada N, Yokoyama Y, et al. Left ventricular obstruction caused by a large hiatal hernia. Echocardiography. 2017; 34: 1254-1256.
- Naoum C, Puranik R, Falk GL, Yiannikas J, Kritharides L. Postprandial left atrial filling is impaired in patients with large hiatal hernia and improves following surgical repair. International journal of cardiology. 2015; 182: 291-293.