
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Hematometrocolpos in chronic vulvovaginal GVHD
Neel Aggerwal1; Manideepa Maji2; Nita Radhakrishnan2*; Ravi Shankar2; Devendra K Gupta1; Sangeeta Tripathy3
1 Department of Pediatric Surgery, Super Speciality Pediatric Hospital and Post Graduate Teaching Institute, Noida, Delhi NCR, India.
2 Department of Pediatric Hematology Oncology, Super Speciality Pediatric Hospital and Post Graduate Teaching Institute, Noida, Delhi NCR, India.
3 Department of Radiodiagnosis, Super Speciality Pediatric Hospital and Post Graduate Teaching Institute, Noida, Delhi NCR, India.
*Corresponding Author: Nita Radhakrishnan
Associate Professor, Department of Pediatric Hematology Oncology, Super Speciality Pediatric Hospital and
Post Graduate Teaching Institute, Noida, Delhi NCR.
Email: nitaradhakrishnan@yahoo.com
Received : Oct 27, 2021
Accepted : Jan 10, 2022
Published : Jan 17, 2022
Archived : www.jcimcr.org
Copyright : © Radhakrishnan N (2022).
Abstract
Chronic Graft-Versus-Host Disease (GvHD) is one of the most common cause of poor quality of life after Hematopoietic Stem Cell Transplantation (HSCT). Chronic GVHD can present with vulvovaginal symptoms which is usually under reported. Only small series have been reported so far and its incidence, pathophysiology, clinical manifestations and management are not well understood. So also, there are currently no vvGVHD screening guidelines for children who undergo HSCT. In this report, we describe our experience of managing an adolescent girl who developed hematometrocolpos as a complication of chronic GVHD after bone marrow transplant.
Citation: Aggerwal N, Maji M, Radhakrishnan N, Shankar R, Gupta DK, et al. Hematometrocolpos in chronic vulvovaginal GVHD. J Clin Images Med Case Rep. 2022; 3(1): 1571.
Introduction
Chronic Graft-Versus-Host Disease (GvHD) is the most common cause of poor quality of life after Hematopoietic Stem Cell Transplantation (HSCT) [1]. Areas most commonly affected are the skin, oral mucosa, eyes, liver, joints, muscles etc. Although Vulvovaginal Gvhd (vvGvHD) typically occurs in the context of GvHD involving another organ system, there are reported cases of isolated vvGvHD [2]. Chronic GVHD is the most common cause of vulvovaginal symptoms after HSCT in adult and pediatric female patients. The reported incidence ranges from 3% to 49%, but the true incidence has not been established [2,3].
We present an adolescent female who developed hematometrocolpos as a complication of chronic GVHD after bone marrow transplant.
Case presentation
14-year girl presented with amenorrhea and pain abdomen while on regular follow up at our center after undergoing Bone Marrow Transplant (BMT). She was diagnosed to have very severe aplastic anemia for which she underwent bone marrow transplant 3 years ago at another center. She received peripheral blood stem cells from her brother and engrafted within 2 weeks. Subsequently she developed chronic skin GVHD for which she has been continued on cyclosporine and has been regularly followed up at our center. She had joint stiffness and contractures which were managed conservatively. Although she had achieved menarche prior to her diagnosis of Aplastic anemia, she developed secondary amenorrhea soon after the diagnosis. Subsequently, her menstrual cycles resumed 2 years after BMT and was uneventful for the initial one year. 1 year later, while on regular follow up, she missed one menstrual cycle. Following this, the next month, she presented to us with severe pain abdomen in the pelvis. Abdominal pain was progressive in nature and was not resolved on any antispasmodic medications. Abdominal examination was apparently normal. In view of chronic skin GVHD and history of recent amenorrhea with pain abdomen, hematometrocolpos was suspected. Perineal examination revealed vulvo-vaginal synechiae.
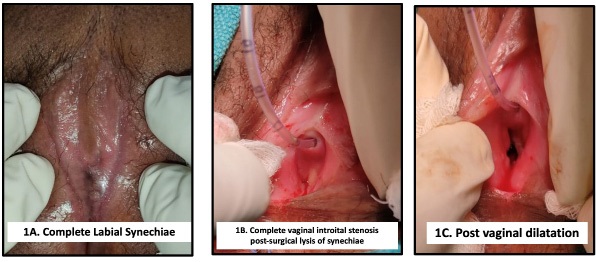
USG pelvis revealed a smooth circumscribed lesion in the pelvis with low level echoes in the area of uterus. She was taken up for examination under anesthesia. Along with labial synechiae, vaginal introitus was completely stenosed with no fluid or discharge seen at the opening (Figure 1A, IB). After surgical lysis of synechia, fibrosed vaginal canal was dilated (Figure 1C). Proximal vagina was patent, with fibrosis appreciated in distal one third of vagina only. 300 ml of menstrual blood was drained from the hematometrocolpos. Post operatively, patient was managed with vaginal dilations in combination with topical estrogen cream once a day for initial two weeks which were gradually tapered. She has been continued on regular vaginal dilatation and topical estrogen since then. Her menstrual cycle resumed the following month and currently she is pain free.
Discussion
GvHD is believed to be a complex immune response, primarily T-cell mediated, in which the grafted donor cells recognize the host as foreign [3]. From the wider literature, some including pediatric patients, isolated vvGVHD is rare, typically it occurs in the context of current or past GVHD involving another organ system, most commonly skin (90 % of cases), oral mucosa, or eyes [2]. vvGvHD is a difficult to diagnose disease which physicians may not be familiar with [3].
Genital GvHD presents at a median of 7–10 months after HCT, but signs and symptoms can also develop late [4]. Classically, GvHD has been classified as acute and chronic GvHD, based on whether symptoms developed within 100 days after the transplant or later. Currently, the number of days after the transplant is not sufficient to differentiate acute from chronic GvHD [3]. Among patients with vvGVHD, predominant symptoms are vulvar pain, dysuria, vulvar itching, urinary incontinence, urinary urgency and frequency etc. The most common exam findings are vulvaradhesions/agglutination, vulvar atrophy, labial erosions, and vestibular pain on exam [2].
A classification of genital GVHD is currently used (minimal, moderate, severe) [5]. The 2014 National Institutes of Health recommendations and scoring system primarily reflect clinical signs rather than severity of symptoms, ranging from score 0 (no signs) to score 3 (severe signs) such that whether patients report symptoms orhave discomfort with exam is not necessary for scoring disease severity [4] (Table 1). Our patient had no discomfort or genital symptoms post BMT apart from amenorrhea. When menstrual cycle resumed 2 years after BMT, she had normal menses for initial one year. Later, abdominal pain and detection of hematometrocolpos was followed by perineal examination which revealed introital stenosis, labial synechiae and complete vaginal obliteration as severe vvGvHD, which needed surgical intervention and couldn’t be managed with topical treatment [6]. According to Stratton scale and National Institute of Health (NIH) guidelines our case fulfilled the criteria of grade III (severe) vulvovaginal GVHD due to presence of introital stenosis, vaginal synechiae, hematometra and complete vaginal closure.
Table 1: Grading of genital chronic GvHD
Classification |
Grade 0 |
Grade 1 |
Grade 2 |
Grade 3 |
NIH consensus criteria genital specific scoring |
No signs |
Mild signs and females may have symptoms with or without discomfort on exam |
Moderate signs and may have symtoms with discomfort on exam |
Severe signs with or without symptoms |
Genital exam scoring |
Females |
Grade 1 (mild) |
Grade 2 (moderate) |
Grade 3 (severe) |
|
Males |
Mild |
Moderate |
Severe |
Despite the first report of vulvovaginal cGvHD in 1982, only small series have focused on the female lower genital tract. Its incidence, pathophysiology, clinical manifestations and management are not well understood [4]. There are currently no vvGVHD screening guidelines for post-HSCT children. Furthermore, there are no studies detailing vulvovaginal complaints and genitalexamination patterns of post-HSCT children who already have a diagnosis of GVHD of any organ system, and are thus at high risk of vvGVHD [2]. Routine gynecological screening should be recommended for pediatric and adolescent patient in the context of severe GVHD patient to reduce the morbidity. Another concern in vvGVHD is the difficult in using prolonged topical immune suppression. This could lead to reactivation of human papilloma virus infection which can lead to premalignant and malignant changes in the cervix, vulva and vagina [7].
Genital GvHD underestimates the true magnitude of this problem, as patients frequently under-report orneglect symptoms and sexual problems, and clinicians underdiagnose this condition [4]. Although the rates of cGVHD after HSCT are lower in the pediatric population than in adults, cGVHD remains a significant cause of morbidity and mortality [8]. Genital manifestations of chronic GvHD are rare and may be underestimated. Because mild chronic GvHD of the vulva or vagina may occasionally be asymptomatic and detected only on examination, genitalcare is need in recepients of allogeneic HSCT [3].
Conclusion
Genital GVHD can be devastating in its presentation, because it affects sexuality and fertility. Genital symptoms might not be readily reported by patients, even during longterm follow-up. Further recognition of symptoms and regular follow-up can help improve the detection and facilitate early treatment of genital GvHD. This can significantly improve the quality of life and morbidity of surgical interventions for late complications.
Author contribution: MM, RS and NR have been involved in her diagnosis and management. NA and DKG managed the surgical condition. ST was involved in the radiological diagnosis. All were involved in the preparation of the manuscript and its revisions.
References
- Bhushan V, Collins R: Chronic graft-vs-host disease. JAMA. 2003; 290: 2599.
- Allen SM, Liang CS, Chesnokova, et al. Patterns of Genital Examination and Vulvovaginal Graft-Versus-Host Disease in a Pediatric Post-Hematopoietic Stem Cell Transplant Population. J Pediatr Adolesc Gynecol. xxx. 2020; 1-e9
- Kim TH, Lee HH, Chung SH. Hematocolpos as a complication of chronic graft-versus-host disease. Taiwanese Journal of Obstetrics & Gynecology. 2012; 51: 292-e293.
- Hamilton BK, Goje O, Savani BN, et al. Clinical management of genital chronic GvHD. Bone Marrow Transplantation. 2017; 52: 803–810.
- Riera C, Deroover Y, Marechal M. Eur. J. Gynaec. Severe vaginal chronic Graft-Versus-Host Disease (GVHD). Two cases with late onset and literature review. Oncol. 2010; ISSN: 0392-2936 XXXI, n. 6.
- Resolution of Hematocolpos in Adolescents Affected with Graft vs Host Disease. Michala L, Vlachopapadopoulou E, Tsimaris P, et al. J Pediatr Adolesc Gynecol. 2018; 31: 536-e539
- Buchan A, Merideth MA, Childs RW, Stratton P. Novel management of vaginal chronic graft-versus-host disease causing haematometra and haematocolpos. BMJ Case Rep. 2018; 2018: bcr2017222720.
- Lawitschka A, Ball L, Peters C. Nonpharmacologic Treatment of Chronic Graft-versus-Host Disease in Children and Adolescents. Biol Blood Marrow Transplant. 2012; 18: S74-S81.