
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Retrocaval ureter coexisting with renal cell carcinoma: A case report and review of literature
Augustine Obasi Ulebe1*; Anselm Okwudili Obi1,2; Uchechukwu Ugonna Ogbobe1; Chinonso Odo1
1 Department of Surgery, Alex Ekwueme Federal University Teaching Hospital Abakaliki, PMB 102, Abakaliki Ebonyi State, Nigeria.
2 Department of Surgery, Ebonyi State University Abakaliki, Ebonyi State, Nigeria.
*Corresponding Author: Augustine Obasi Ulebe
Department of Surgery, Alex Ekwueme Federal
University Teaching Hospital Abakaliki, PMB 102,
Abakaliki Ebonyi State, Nigeria.
Email: ulebester@yahoo.com
Received : Oct 23, 2021
Accepted : Jan 10, 2022
Published : Jan 17, 2022
Archived : www.jcimcr.org
Copyright : © Ulebe AO (2022).
Abstract
Background: Retrocaval Ureter (RCU) is a rare congenital anomaly that often presents with obstructive changes in the upper urinary tract which may or may not symptomatic. It arises as a result of an aberration in embryologic development of Inferior Vena Cava (IVC). Commonly occurs in isolation but can occur in association with other anomalies. Few studies have reported RCU co-existing with upper tract Transitional Cell Carcinoma (TCC) but there is no literature report so far of its co-existence with Renal Cell Carcinoma (RCC).
Case summary: Hence, we report a case of a 65 year old man with right sided RCC coexisting with RCU. The anomaly was discovered intra-operatively and the patient was offered open right radical nephrectomy with a good post-operative recovery and uneventful follow-up.
Conclusion: Retrocaval ureter is a rare congenital anomaly that may occur in isolation or with other associated conditions. To the best of our knowledge, we report the first case of RCU coexisting with renal cell carcinoma. Proper pre-operative evaluation will help to identify these associated anomalies so as to adopt a holistic approach to patient care in order to ensure good treatment outcome.
Keywords: radical nephrectomy; renal cell carcinoma; retrocaval ureter; nephroureterectomy.
Citation: Ulebe AO, Obi AO, Ogbobe UU, Odo C. Retrocaval ureter coexisting with renal cell carcinoma: A case report and review of literature. J Clin Images Med Case Rep. 2022; 3(1): 1573.
Introduction
Retrocaval Ureter (RCU) is a rare congenital anomaly that often presents with obstructive changes in the upper urinary tract which may or may not be symptomatic. It arises as a result of an aberration in embryologic development of the Inferior Vena Cava (IVC) [1]. The anomaly is commonly seen on the right side but can be left-sided in some cases of situs inversus or IVC duplication [2,3]. Its incidence is approximately 1 /1,100, with a male to female ratio of 2.8 to 1 [1]. Although the anomaly is congenital, patients usually become symptomatic in their 3rd or 4th decade of life [4]. The pathology commonly occurs in isolation [5], but may exist in association with other anomalies in up to 21% of cases [6]. Possible associated anomalies include retroperitoneal fibrosis [7], solitary kidney with or without renovascular hypertension [8,9] horseshoe kidney [10], congenital absence of vas deferens [11] and Goldenhar (Branchial arch) syndrome [12].
Few studies have reported RCU co-existing with upper tract Transitional Cell Carcinoma (TCC) [13,14] but to the best of knowledge, there is no literature report so far of its co-existence with Renal Cell Carcinoma (RCC). Hence, we report a case of a 65 year old man with right sided RCC coexisting with RCU. This may well be the first reported case of RCU coexisting with RCC.
Case summary
A 65 year old man, who presented to our facility with a 2 year history of intermittent total hematuria associated with right flank pain but no mass. There were no history of anorexia, weight loss and lower urinary tract symptoms. Patient was a known hypertensive and diabetic with past history of seizures. He did not smoke or use tobacco in any form.
General and abdominal examinations were unremarkable. He had no ballotable kidneys, palpable liver or spleen. Digital rectal examination revealed moderately enlarged prostate that was smooth surfaced with intact median sulcus.
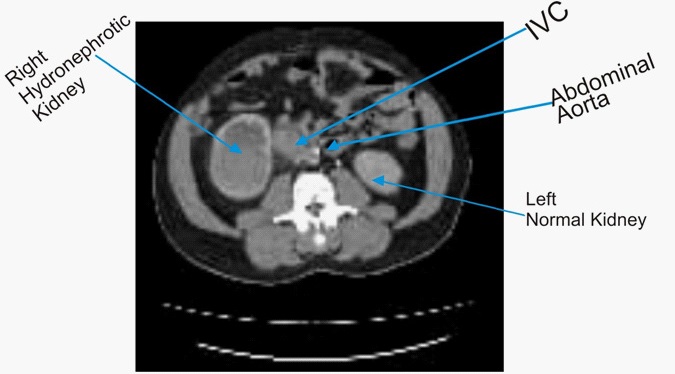
Review of available laboratory and radiological investigation results showed hemoglobin of 12.8 g/dl and total PSA of 10.46 ng/ml. Abdominopelvic USS showed right renal mass (5.25 X 6.70 cm) most likely a renal cell carcinoma and prostate volume of 75.9 ml. The IVU showed right renal mass with hydronephrosis and proximal hydroureter while the CT urography showed pelvi-ureteric mass in the right kidney, likely urothelial tumor, medial displacement of IVC and normal left kidney (Figure 1). Cranial CT scan showed mild cerebral atrophy with no mass lesion and features of rhinosinusitis.
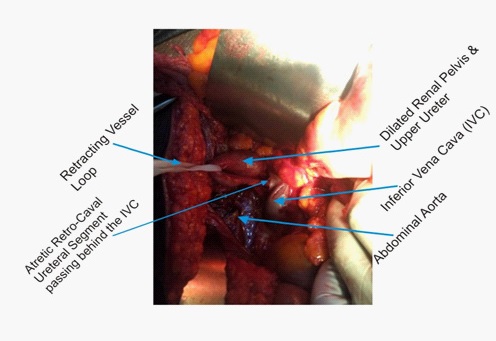
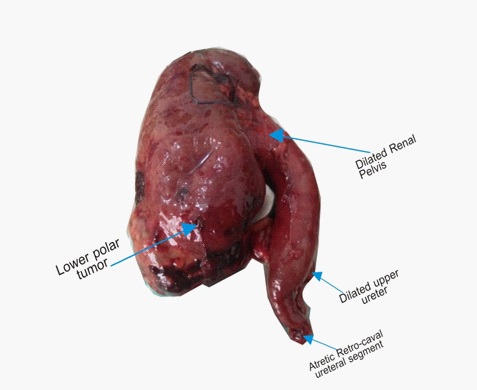
A diagnosis of right RCC with right hydroureteronephrosis, on the background of hypertension, diabetes mellitus and seizure disorder was made. Following appropriate work up, the patient was offered open right radical nephrectomy. At surgery, the patient was found to have a RCC in addition to right RCU with proximal hydrouretero-nephrosis was discovered intraoperatively during the interventional surgical procedure (Figure 2). Post-operative histopathologic examination of the specimen revealed right renal cell carcinoma, papillary variant (Figure 3). The patient had uneventful post-operative recovery. At the time of writing, the patient has had 5 months follow up without incident.
Discussion
Retrocaval ureter was first reported by Hochstetter in 1893 [15]. It arises as a result of an aberration in embryologic development of the Inferior Vena Cava (IVC) between the 6th and the 8th week of gestation [1]. The IVC is formed following the anastomosis and involution of 3 pairs of primordial veins: The Posterior Cardinal Veins (PCVs), The Sub-Cardinal Veins (SCVs) and The Sacro-Cardinal Veins (SaCVs). The right SCV develops into the renal segment of the IVC while the left SCV remains as the left renal vein and left gonadal vein. The SaCVs develop into the common iliac veins while the right PCV forms the right gonadal vein. The right SCV is medial to the developing ureter, resulting in the normal anatomic relation between the IVC and the ureter by the time of birth. A retrocaval ureter results from the persistence of the right PCV as the renal segment of the IVC [1]. This vein is lateral to the ureter, with a ureteral course that crosses posterior and medial to the IVC, emerging between the IVC and the aorta and deviating laterally and caudally on its way to the pelvis.[1]
Bateson and Atkinson [16] in 1969, classified RCU into two types based on the radiological appearance and site of ureteral narrowing. The type I (low loop), seen in about 90% of cases, is characterized by the ureter crossing behind the IVC at the level of the 3rd lumbar vertebra. On retrograde pyelogram, it shows a fish hook (S shaped) or reversed “J” deformity at the point of obstruction. Marked hydronephrosis is seen in 50% of cases. In the less common type II (high loop), the renal pelvis and up per ureter lie horizontally with the retrocaval segment of the ureter at the same level as the renal pelvis (segment becomes retrocaval at renal pelvis). There is less medial deviation of the ureteral segment. The IVC is encircled in a smooth curve (sickle shaped curve) as seen in retrograde pyelogram with mild hydronephrosis. Type II is less common and accounts for 10% of all cases [16].
Our patient had type I variety with moderate hydronephrosis. Mode of presentation is variable, ranging from asymptomatic cases with incidental discovery on imaging to presentation with a variety of symptoms. Our patient presented with haematuria and right flank pain which is similar to the case reported by Andre Cardoso et al. [14] and Mayuri A et al. [17].
Diagnosis of RCU can be made on ultrasonography, intravenous urography, retrograde and antegrade uretero-pyelography with confirmation by computed tomographic urography and magnetic resonance urography. Each of these imaging modalities has its own merits and demerits. Diagnosis is often suggested by the typical radiological features mentioned above. However in this patient, the classical reversed “J” sign was not clearly evident on various pre-op radiological investigations. Hence, the diagnosis of right renal tumor was made missing the coexisting RCU, which was detected intra-operatively. This is similar to the experience by Obi AO et al. [18] that previously reported 2 cases of RCU with the anomaly discovered intra-operatively in both patients, despite some radiologic investigations done to aid the pre-operative diagnosis. Poor imaging quality and oversight error in imaging interpretation might have contributed to failure to detect RCU pre-operatively. This diagnostic dilemma may further be compounded if this anomaly coexists with other disease conditions like RCC as is seen in our index patient. The RCU is a rare condition and often asymptomatic, hence a high index of suspicion is required to diagnose the condition pre-operatively.
Various concomitant anomalies have been associated with RCU [6]. Our patient had RCU coexisting with RCC. There is no literature publication of such an association in the past to the best of our knowledge. It is not clear whether there is any causal relationship between the two pathologies or whether this is a coincidental finding. However, few cases of RCU have been reported to co-exist with upper tract Transitional Cell Carcinoma (TCC) [15,16]. Causes are unknown but upper urinary tract obstruction, urinary stasis and increased risk of recurrent UTI with stone formation and prolonged contact time of urinary carcinogens with upper tract urothelium as seen in RCU have been postulated as the possible predisposing factors [15,16]. Whether this is also applicable in cases of RCU coexisting with RCC is not clear considering the fact that concomitant upper tract malignancies including RCC are rare in patients with RCU. Considering rarity of RCC coexisting with RCU, one may be tempted to say that this is coincidental finding in our patient. Our patient also has other co-morbidities like hypertension, diabetes mellitus and seizures. Cranial CT scan in our patient ruled out the possibility of brain metastasis with space occupying lesions from the RCC as the cause of the seizures. The patient had good symptom control with antiepileptics. Tanaka et al [8] reported renovascular hypertension in a patient with a solitary kidney. The hypertension in our patient is a coincidental finding as it persisted even after surgical intervention.
Asymptomatic patients with RCU can be managed expectantly and followed up conservatively. However, symptomatic cases with complications like significant obstruction, infection, urolithiasis, renal impairment or increasing hydronephrosis should be treated. Surgical treatment options include ureteropyelostomy and uretero-ureterostomy with or without excision of retrocaval segment. This can be achieved through open or laparoscopic approaches. Simple nephrectomy may be required in patients with nonfunctioning kidney. However, our patient was offered right radical nephrectomy which is the standard of care for RCC. Histological diagnosis of papillary RCC was made. The patient had a good post-operative outcome and uneventful follow-up.
Conclusion
Retrocaval ureter is a rare congenital anomaly that may occur in isolation or with other associated conditions. To the best of our knowledge, we report the first case of retrocaval ureter coexisting with renal cell carcinoma. Such associated anomalies may alter the treatment approach from simple to radical operative procedure. Proper pre-operative evaluation will help to identify these associated anomalies so as to adopt a holistic approach to patient care in order to ensure good treatment outcome. It is a rare congenital anomaly that requires a high index of clinical suspicion to enhance pre-operative diagnosis.
References
- Lesma A, Bocciardi A, Rigatti P: Circumcaval ureter: Embryology. Eur Urol Suppl. 2006; 5: 444-448.
- Wang LT, Lo HC, Yu DS, Sun GH, Wu CC, Fong CJ. Ureteral obstruction caused by a duplicated anomaly of inferior vena cava. Int J Urol. 2005; 12: 842-844.
- Gramegna V, Madaro A, Pellegrini F, Capizzi S, Romano O, et al. A rare case of retrocaval ureter associated with persistent left vena cava. Urol Int. 2003; 70: 337-348.
- Rubinstein I, Cavalcanti AG, Canalini AF, Freitas MA, Accioly PM. Left retrocaval ureter associated with inferior vena caval duplication. J Urol. 1999; 162: 1373-1384.
- Aliasghar Y, Mohamadali M R, Behzad, Hassan A. Retrocaval Ureter: A Study of 13 Cases Urol J (Tehran). 2006; 3: 175-179.
- Perimenis P, Gyftopoulos K, Athanasopoulos A, Pastromas V, Barbalias G. Retrocaval ureter and associated abnormalities. Int Urol Nephrol. 2002; 33: 19-22.
- Arriola PM, el-Droubi H, Dahlen CP. Combined retrocaval ureter and retroperitoneal fibrosis: Report of a case. J Urol. 1979; 121: 107-8.
- Tanaka K, Akimoto S, Kozuma T. Renovascular hypertension with a solitary kidney associated with retrocaval ureter: A case report. Nippon Geka Gakkai Zasshi. 1984; 85: 849-54. Japanese.
- Altland H, Molitor D. Retrocaval ureter with unilateral agenesis of the kidney. Rofo. 1983; 138: 106-109.
- Shigeta M, Nakamoto T, Nakahara M, Hiromoto N, Usui T. Horseshoe kidney with retrocaval ureter and ureteropelvic junction obstruction: A case report. Int J Urol. 1997; 4: 206-208.
- Baba Y, Ishizu K, Nakamura K, Ueno T, Takihara H, Sakatoku J. et al. Congenital absence of the vas deferens associated with retrocaval ureter: A case report. Hinyokika Kiyo. 1991; 37: 175-177.
- Ishitoya S, Arai Y, Waki K, Okubo K, Suzuki Y. Left retrocaval ureter associated with the Goldenhar syndrome (branchial arch syndrome). J Urol. 1997; 158: 572-573.
- Fillo J, Cervenakov I, Mardiak J, Szeiff S, Kopecny M, Labas P, et al. Retrocaval ureter with ureteral carcinoma. Bratisl Lek Listy. 2003; 104: 408-410.
- Andre C T, Correia R S, Manuel C M, Almeida R P. Right Circumcaval Ureter and Renal Pelvis Urothelial Carcinoma. Curr Urol. 2009; 3: 100–102.
- Hochstetter F. Beitrage zur entwicklungsgeschichte des venensystems der amnioten: III. Sauger Morph Jahrb. 1893; 20: 542.
- Bateson EM, Atkinson D. Circumcaval ureter: a new classification. Clin Radiol. 1969; 20: 173-177.
- Mayuri A. Kamble, Thawait P, Ashok T. Kamble. Retrocaval ureter: a rare congenital anomaly presenting as renal colic with hematuria. Int Surg J. 2014; 1: 21-24.
- Obi A O, Udeh F N and Ndubueze E. Retrocaval Ureter; A rare Cause of Hydronephrosis. Report of 2 cases and Literature Review. Nigerian Journal of Surgical Sciences. 2009; 19: 72-76.