
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 2
Resection arthroplasty of the proximal humerus following chondrosarcoma removal and reconstructive failure: A case report with 22 year follow-up
Maria LaMontagne1; Timothy A Damron2*
1 Upstate Medical University, 7135 Boardwalk Drive, Cicero, NY 13039, USA.
2 State University of New York, Syracuse Upstate Bone and Joint Center, 6620 Fly Road, East Syracuse, NY 13057, USA.
*Corresponding Author: Timothy Damron
State University of New York, Syracuse Upstate Bone
and Joint Center, 6620 Fly Road, East Syracuse, NY
13057, USA.
Email: damront@upstate.edu
Received : Dec 02, 2021
Accepted : Jan 11, 2022
Published : Jan 18, 2022
Archived : www.jcimcr.org
Copyright : © Damron T (2022).
Abstract
Introduction: Proximal humeral reconstructive alternatives in orthopedic oncology are well described, but the literature regarding post-failure salvage is sparse. This report details a multiply failed humeral reconstruction that ultimately resulted in resection arthroplasty. Although initial tumor resection was treated with an intercalary reconstruction, this case is unique in that its sequelae are equally applicable to failures of proximal humeral reconstruction.
Case presentation: We report a 61-year-old Caucasian woman with ultimate removal of a second proximal humeral reconstruction twenty-two years after initial grade I chondrosarcoma resection, leaving essentially a shoulder resection arthroplasty
Conclusion: The patient’s acceptance of resection arthroplasty in this case suggests that not all failures of proximal humeral major reconstructive procedures need to be revised to another reconstruction. Resection arthroplasty is much less complex than revision surgery, requires little healing time, expedites recovery, minimizes subsequent further complications and allows for excellent pain relief. Resection arthroplasty may be a plausible approach after failed orthopedic oncology humeral reconstruction in carefully selected patients.
Keywords: chondrosarcoma; resection arthroplasty; reconstruction; musculoskeletal tumor; intercalary allograft; proximal humerus; shoulder; shoulder arthroplasty
Citation: LaMontagne M, Damron TA. Resection arthroplasty of the proximal humerus following chondrosarcoma removal and reconstructive failure: A case report with 22 year follow-up. J Clin Images Med Case Rep. 2022; 3(1): 1578.
Introduction
Failures of orthopedic oncology reconstructions include infection, fracture, subluxation, dislocation, component loosening, tumor progression and non-union [1]. Failures of proximal humeral reconstructions are no exception [2]. When the proximal humerus can be spared, intercalary humeral allografts are commonly utilized but have failure rates of 15% [3]. Salvage options of failed reconstructions include revision or conversion to a different reconstruction. Both have been reported, but there is sparse literature on resection arthroplasty. We report a 61- year-old woman with ultimate removal of a second proximal humeral reconstruction after index chondrosarcoma resection, leaving essentially a shoulder resection arthroplasty.
Case presentation
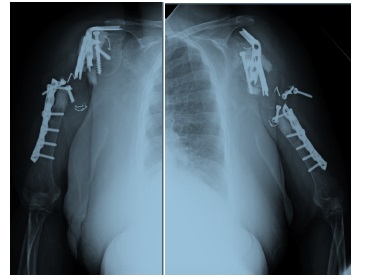
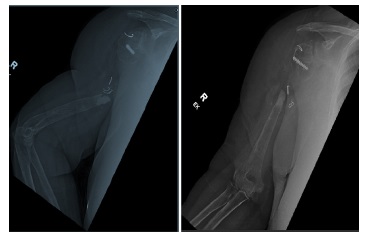
A 42-year-old woman underwent en-bloc resection of a very proximal right humeral diaphyseal grade I chondrosarcoma 22 years ago with intercalary allograft reconstruction using plate and screw fixation. This aggressive approach was selected because extended intralesional curettage and cementation was not yet a widely accepted treatment for low grade chondrosarcoma. An intercalary proximal humeral segment with the tumor was removed, sparing only the humeral head, and due to the limited remaining epiphyseal bone and compromised rotator cuff attachments, a GORE-TEX Vascular Graft (Flagstaff, AZ) was used about the remaining humerus and allograft for soft tissue reconstruction. The intercalary allograft segment was supplemented with intramedullary Simplex Tobramycin bone cement (Howmedica Inc. Rutherford, N.J.) to minimize fracture and resorption. A proximal humeral 90° blade plate was supplemented by two other plates and 18-gauge wire. Two months postoperatively, the patient presented with pain. X-rays revealed windshield wiping of the blade plate, indicating early proximal fixation failure. Revision was undertaken. The cavity formed due to windshield wipering of the blade plate was curetted, and a wedge of cortical cancellous iliac crest was tamped into the space distal to the blade plate followed by supplemental screw fixation. Fifteen months later, the patient presented with pain, and motion at the non-union site. Radiographs showed further windshield wiper effect of the blade plate with broken wire, but the patient declined revision at that time and again a year later despite worsening pain. Nineteen years postoperatively (age 61), patient returned again with worsening pain. Physical examination showed accessory motion within the proximal one-third of the humerus, palpable hardware, and flail shoulder. X-rays revealed complete osteolysis of entire intercalary allograft construct with broken hardware. Only a small piece of residual humeral head remained with posterior subluxation and no other bone to the distal one-third of the native humerus. The proximal portion of the blade plate eroded the undersurface of the acromial process and glenoid cavity. Laboratory testing showed an elevated ESR and CRP, with a normal WBC. The patient declined surgical intervention. Later that year, the patient opted for hardware removal, but declined reconstruction. Hence, broken plates, free-floating screws, and cement fragments were removed, but no allograft remained. Pathology review showed no tumor recurrence or acute inflammation and cultures were negative. Twenty-two years after initial presentation, the patient reports resection arthroplasty provided her 100% pain relief. She has profound functional limitations and is unable to rake, hold heavy objects, lift with the arm, or abduct the arm past 15 degrees. Her MSTS score is 14/30, with motion 0/5 for motion, 5/5 pain, 0/5 stability, 5/5 deformity, strength 0/5, functional disabilty 1/5, andemotional acceptance 3/5. X-rays at latest follow-up showed no changes (Figure 3).

Discussion
Intercalary humeral reconstructions carry their own risks as illustrated by this case. Complications of both intercalary and proximal humeral reconstruction are relevant in this case as it ultimately led to proximal humeral resection arthroplasty. Results of intercalary humeral allograft reconstructions are imperfect [3]. Ognik et. Al reported 27% revision rate of intercalary allografts with median three years to revision surgery, as seen with our patient [4]. Common causes of intercalary allograft failure include nonunion (40%), fracture (29%), and infection (14%), with reoperation in 70% of patients [3]. When the intercalary humeral allograft fails proximally, the humeral head may have to be resected, creating an intra-articular proximal humeral defect. Proximal humeral allograft and osteoarticular allograft reconstructions complication rates are also high. A systematic review showed MSTS (Musculoskeletal Tumor Society) scores of 57% to 91% following allograft-prosthesis composite reconstruction [2]. Although recent reports with reverse total shoulder APC have shown improvements, most reconstructive options limit shoulder mobility and function. In a systematic review of proximal humeral reconstruction options (reverse shoulder arthroplasty, hemiarthroplasty, megaprosthesis, APC, OAA, allograft arthrodesis and autograft arthrodesis) following proximal humeral tumor resection, allograft containing constructs had the highest rates of mechanical failure [5]. Failure rates of allografts are significantly higher among patients over eighteen, and patients undergoing diaphyseal reconstruction3. Bus et. al also found when analyzing time to failure for allograft reconstructions, bridging plate fixation and age greater than eighteen years old were the top factors [3]. Published reports of humeral revision options are sparse. While intercalary graft failure is common, Mourikis et. al reported 77% overall success following revision [6]. Options for revision include supplemental autograft (vascularized fibula or iliac crest bone graft), repeat allograft reconstruction or conversion to an endoprosthesis. Ippolito et. al reported 88% allograft preservation and 98% limb salvage after autograft supplementation of intercalary allograft reconstruction [7]. Although endoprosthesis salvage of failed intercalary allograft is an acceptable alternative, long-term durability is dubious, and risks include abductor muscle damage and inadequate proximal fixation [8,9].
In the proximal humerus, failure due to subluxation or dislocation can be salvaged with conversion to a reverse shoulder arthroplasty with good functional result [10]. In a single case report, an osteoarticular allograft reconstruction following proximal humeral osteosarcoma resection required three subsequent procedures to address non-union and hardware failure, ultimately requiring intramedullary nail fixation and vascularized fibular autograft [11]. Although no literature regarding resection arthroplasty for failed humeral reconstructions after tumor resection was found, relevant articles were identified in orthopedic trauma and arthroplasty. A systematic review comparing the results of exchange arthroplasty to permanent spacer or resection arthroplasty of shoulder prosthesis found no significant difference in postoperative function among the three modalities [12]. Although indications for shoulder resection arthroplasty are not absolute, resection arthroplasty is generally considered a salvage procedure for failed replacement, infection, or septic arthritis [13]. A retrospective study following failed nononcologic shoulder arthroplasty found 71% of patients were satisfied with the outcome of resection arthroplasty, and 86% would make the choice again [14]. Similarly, Pelligrini et, al studied two cohorts who underwent two-stage revision of shoulder prosthesis for non-oncology indications compared to placement of a permanent antibiotic spacer following periprosthetic shoulder infection. Follow up demonstrated no significant difference found regarding infection clearance or functional ability, but a higher complication rate in the two-stage revision cohort [15]. Results suggested two-stage revision may be favorable in younger adults, yet antibiotic spacer placement may provide satisfactory functionality for older patients with fewer functional needs [15]. Risopli et. al studied [18] nononcologic patients who underwent resection arthroplasty of the shoulder following indications of active infection, chronic pain and glenohumeral instability, concluding that this approach provided significant pain relief in the majority of patients, with 55% reporting no or little pain at follow up, but 14 of 18 with profound functional limitations post-resection [13]. Our patient also had excellent pain relief, and although she rated emotional acceptance on the MSTS scale as 1/5, she declined repeated offers for revision arthroplasty.
Conclusion
Resection arthroplasty following failed oncology reconstructions of the proximal humerus or, in this case, the proximal humeral diaphysis, to our knowledge, has not been previously reported as a salvage procedure. Resection arthroplasty is much less complex than revision surgery, requires little healing time, expedites recovery, minimizes subsequent further complications and allows for excellent pain relief. As reported in trauma and shoulder arthroplasty literature, good pain relief and acceptable patient satisfaction can be achieved, albeit with profound functional loss.
Clinical message
Resection arthroplasty may be a plausible approach after failed orthopedic oncology humeral reconstruction in carefully selected patients. This surgical alternative should be considered for patients with multiple reconstructive failures who are still experiencing pain and desire a less intensive surgical option with quicker recovery time.
Declarations
Patient consent: The authors confirm that patient consent was obtained.
Author contributions
ML: Collection of relevant source material, analysis of sources and writing of the manuscript.
TD: Conception of manuscript, supervision of research completed by ML, writing and editing of manuscript, selection of figures. All authors have read and approved the manuscript.
Acknowledgments: The authors wish to acknowledge Tina Craig, our research coordinator, for her assistance in patient contact and communication. Funding for this project was obtained through a grant from the William Smythe Cancer Fund of the Upstate Medical University Research Foundation.
Disclosures: None relevant to this publication.
References
- Henderson ER, O’Connor MI, Ruggieri P, et al. Classification of failure of limb salvage after reconstructive surgery for bone tumours : a modified system Including biological and expandable reconstructions. Bone Joint J. 2014; 96-B(11): 1436-1440.
- Teunis T, Nota SP, Hornicek FJ, Schwab JH, Lozano-Calderón SA. Outcome after reconstruction of the proximal humerus for tumor resection: a systematic review. Clin Orthop Relat Res. 2014; 472(7): 2245-2253.
- Bus MPA, Dijkstra PDS, MD, PhD, et al. Intercalary Allograft Reconstructions Following Resection of Primary Bone Tumors: A Nationwide Multicenter Study. J Bone Joint Surg Am. 2014; 96(4): 26.
- Ogink PT, Teunissen FR, Massier JR, Raskin KA, Schwab JH, Lozano-Calderon SA. Allograft reconstruction of the humerus: Complications and revision surgery. J Surg Oncol. 2019; 119(3): 329-335.
- Dubina A, Shiu B, Gilotra M, Hasan SA, Lerman D, Ng VY. What is the Optimal Reconstruction Option after the Resection of Proximal Humeral Tumors? A Systematic Review. Open Orthop J. 2017; 11: 203-211.
- Mourikis A, Mankin HJ, Hornicek FJ, Raskin KA. Treatment of proximal humeral chondrosarcoma with resection and allograft. J Shoulder Elbow Surg. 2007; 16(5): 519-524.
- Ippolito JA, Martinez M, Thomson JE, et al. Complications following allograft reconstruction for primary bone tumors: Considerations for management. Journal of Orthopaedics. 2019; 16(1): 49-54.
- Squire G, Grundy TJ, Ferran NA, Harper WM, Ashford RU. Longterm survival of proximal humerus allografts for reconstruction following resection of malignant bone tumours. Acta Orthop Belg. 2013; 79(3): 260-265.
- Wei R, Guo W, Yang R, Tang X, Yang Y, Ji T. Plate-prosthesis composite reconstruction after large segmental resection of proximal humeral tumors. Medicine. 2019; 98(22).
- Chauhan VS, Vaish A, Vaishya R. Reverse shoulder arthroplasty after failed megaprosthesis for osteosarcoma of the proximal humerus: A case report and review of literature. J Clin Orthop Trauma. 2019; 10(3): 526-530.
- Yuan BJ. Repeated Failure of Fixation of an Allograft Humerus Reconstruction. International Congress for Joint ReconstructionInternet. Updated 2013 Sept 30; cited 2020 Nov 16. Available from: https://icjr.net/articles/repeated-failure-offixation-of-anallograft-humerus-reconstruction.
- George DA, Volpin A, Scarponi S, Haddad FS, Romanò CL. Does exchange arthroplasty of an infected shoulder prosthesis provide better eradication rate and better functional outcome, compared to a permanent spacer or resection arthroplasty? a systematic review. BMC Musculoskelet Disord. 2016; 17(52).
- Rispoli DM, Sperling JW, Athwal GS, Schleck CD, Cofield RH. Pain relief and functional results after resection arthroplasty of the shoulder. J Bone Joint Surg Br. 2007; 89-B(9): 1184-1187.
- Stevens NM, Kim HM, Armstrong AD. Functional outcomes after shoulder resection: the patient’s perspective. J Shoulder Elbow Surg. 2015; 24(9).
- Pellegrini A, Legnani C, Macchi V, Meani E. Two-stage revision shoulder prosthesis vs. permanent articulating antibiotic spacer in the treatment of periprosthetic shoulder infections. Orthop Traumatol Surg Res. 2019; 105(2): 237-240.