
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Ovarian steroid cell tumor, not otherwise specific, causes Cushing syndrome in 6 years old girl: A case report
Versha Rani Rai; Karishma Rahak*; Maira Riaz; Shazia Mahar; Ikramullah Shaikh; Shafqat; Mohsina Noor Ibrahim
National Institute of Child Health, Karachi, Pakistan.
*Corresponding Author: Kirishma Rahak
National Institute of Child Health, Karachi, Pakistan.
Email: dr.rahak@yahoo.com
Received : Dec 23, 2021
Accepted : Jan 13, 2022
Published : Jan 20, 2022
Archived : www.jcimcr.org
Copyright : © Rahak K (2022).
Abstract
We report a case of 6 years old girl with ovarian Steroid Cell Tumor, Not Otherwise Specific (SCT-NOS). She was admitted to the hospital with increased weight gain, hypertrichosis, and cushingoid facies in form of prominent cheecks, moon facies with dorsocervical fat pad, obese built, acanthosis nigricans on back of neck and marked hirsutism.
Initial workup showed raised level if cortisol with loss of diurnal rhythm, and undetectable Plasma ACTH levels, increased testosterone levels. Ultrasound revealed left sided adnexal mass having no flow inside, which was later confirmed on CT as neoplastic lesion of left ovary measuring 6.9 X 8.1 X 4.9 cm. The patient underwent left oophorectomy and pathological examination showed steroid cell tumour, limited to ovary and negative for malignancy. She was kept on IV hydrocortisone preop and post operatively and antihypertensives. After tumor resection her testosterone and cortisol returned to normal levels.
Keywords: steroid cell tumor; not otherwise specific; cushing syndrome; ovarian mass.
Citation: Rai RV, Rahak K, Riaz M, Mahar S, Shaikh, et al. Ovarian steroid cell tumor, not otherwise specific, causes Cushing Syndrome in 6 years old girl: A case report. J Clin Images Med Case Rep. 2022; 3(1): 1591.
Introduction
SCT-NOS in children and adolescents are extremely rare, with only about 9 cases found in a PubMed search, and first case reported in our country. In some pediatric SCT-NOS cases, the functional features of steroid hormone-secreting cells produce characteristic clinical signs of virilization and Cushing’s syndrome. The majority of these tumors have a benign character, but a small portion of them behave in a malignant manner. In this report we describe the case of a 6 year old girl presented with increased weight gain, hirsutism, cushingoidfacies. SCTNOS of the ovary should be considered in cases of childhood virilization. In addition, treatment for this tumor type and followup regarding endocrinological symptoms are further explained in the discussion section.
Case report
A 6 year old female patient admitted with complains of weight gain and hirsutism for past 10 months. On examination she had obvious cushingoid facies (Figure 1A), facial hair growth, hypertrichosis (Figure 1B), dorsocervical fat pad, acanthosis nigracans and marked hirsutism with ferriman Gallwey score of 25.
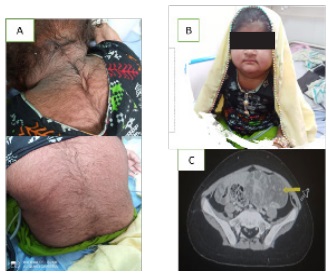
Her blood pressure was >99th centile whereas tanner staging was P3 A1 B1.
Abdominal ultrasound detected left sided adnexal mass having no flow inside. On CT abdomen it was a left adnexal mass of 6.9 X 8.1 X 4.9 cm (CC X TS X AP measurements. Investigation showed increased level of morning cortisol 28.10 ug/dl with loss of diurnal rhythm and undetected plasma ACTH. Testosterone level 118.8 ng/dl which was four times normal. Thyroid profile, FSH, LH, beta. HCG, alpha fetoprotein all were in normal ranges.
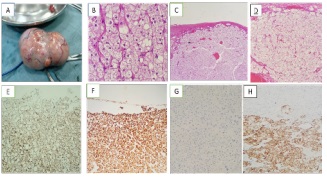
She underwent left oophorectomy. The surface of tumor was smooth without adhesions to surrounding area (Figure 2A). Right ovary and peritonium was normal on intraopertative finding. Mass was present with findings of intact capsule and dilated vessels (Figure 2C). Histopathological report revealed steroid cell tumour NOS (Not Otherwise Specified) which was negative for malignancy. Immunohistochemical strain performed which shows positive inhibin (Figure 2F), calretenin (Figure 2E), Melanin A (Figure 2H) and CD68. She was kept on intravenous hydrocortisone pre and post operative day to avoid adrenal crises. Postoperatively her levels of cortisol and testosterone became normal.
Tab captopril was started for high BP. Postoperatively cortisol and testosterone levels returned to normal level. 4 months after treatment the patient has been without tumor recurrence, in outpatient follow up. Signs of cushing syndrome and hirsutism have improved with no evidence of postoperstive adrenal insufficiency.
Discussion
Imaging features of HCC on MRI
Steroid cell tumors of the ovary account for 0.1% of all ovarian tumors and are rarest tumours that cause virilization in children [1].
These tumors are divided into three subtypes according to their cells of origin: stromal luteoma, leydig cell tumor and steroid cell tumor, Not Otherwise Specified (NOS). Among these subtypes, the steroid cell tumors, NOS constitute for about 56% of steroid cell tumors [2]. Commonly, androgenic manifestations in form of virilisation particularly hirsutism are seen in these tumors as they secrete hormones like androstenedione, α hydroxyprogesterone, and testosterone [3]. However there may be features of cushing syndrome as seen in our case due to increased secretion of cortisol. Macroscopically these tumors are yellow orange due to high fat content. The tumor is commonly confined to ovary but rare presentation of extraovarian steroid cell tumor have been found [4]. It is distinguished from leydig cell tumour by absence of reinke crystals in cytoplasm which is hallmark of leydig cell tumor. Definitive diagnosis is made by histology. Mostly these tumors are unilateral an benign, however 25-43% of steroid cell tumors are clinically malignant with 20% cases exhibiting metastasis outside the ovary [5]. A study by hayes and scully [6] documented five pathological features indicative of malignancy as shown in Table below.
In our case, there were no mitotic activity, cytologicatypia, hemorrhage or necrosis, tumor size was 4.1 X 3.5 cm. The treatment depends upon age of patient, clinical features, tumor histology, surgical staging and desire to preserve fertility. In younger age girls conservative surgery with unilateral oophorectomy is performed as in our case because there were no signs of malignant potential. Her harmone levels rapidly declined to normal levels after surgery. Neither relapse nor metastasis was detected posoperatively at 6th month evaluation.
Microscopic features |
% chance of malignancy |
1) Two or more mitosis per 10 high-power field. |
92 |
2) Necrosis |
86 |
3) Size of tumor more than 7cm |
78 |
4) Hemorrhage |
77 |
5) Grade 2 or 3 nuclear atypia |
64 |
Conclusion
Steroid cell tumors are rarely found in childhood. This case emphasizes the importance of early consideration of tumor causing cushingoid features and virilization. Early diagnosis is possible with clinical correlation along with histopathlogy of tumor mass in most cases. Definative treatment is with surgical resection of mass and further management is decided on tumor pathology.
References
- Balu L, Gasc JM, Boccon Gibod L, et al. Arterialhypertension and ovarian tumour in a girl: What is the link? Nephrol Dial Transplant. 2005; 20: 231-234.
- Patricia Alves, Ines Sa, Miguel Brito, Cátia Carnide, Osvaldo Moutinho. An Early Diagnosis of an Ovarian Steroid Cell Tumor Not Otherwise Specified in a Woman. Hindawi Case Reports in Obstetrics and Gynecology; 2019: 1-3.
- Baloglu A, Bezircioglu I, Cetinkaya B, Karci L, Bicer M, et al. Development of secondary ovarian lesions after hysterectomy without oophorectomy versus unilateral oophorectomy for benign conditions: A retrospective analysis of patients during a nine-year period of observation. Clin Exp Obstet Gynecol. 2010; 37.
- Dinc G, Saygin I, Kart C, Mungan S, Guven S, Guven E, et al. A rare case of postmenopausal severe virilization: Ovarian steroid celltumour, not otherwise specified. J Cases Obstet Gynecol. 2016; 3: 19-21.
- Jiang W, Tao X, Fang F, Zhang S, Xu C. “Benign and malignant ovarian steroid cell tumors, not otherwise specified: Casestudies, comparison, and review of the literature,” Journal of Ovarian Research. 2013; 6: 53.
- Vulink AJ, Vermes I, Kuijper P, ten Cate LN, Schutter EM. “Steroid cell tumour not otherwise specified duringpregnancy: A case report and diagnostic work-up for virilisation in a pregnant patient, “European Journal of Obstetrics & Gynecology and Reproductive Biology. 2004; 12: 221–227.