
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Middle - aortic syndrome with a thrombus in the renal artery
H Foudad1*; I Bouague Li1; K Selmani2; A Trichine1
1 Department of Cardiology, Military Hospital of Constantine, Algeria
2 Department of Radiology, Military Hospital of Constantine, Algeria.
*Corresponding Author: H Foudad
Department of Cardiology, Military City of Military Hospital, Military Hospital of Constantine, Algeria.
Email: hfoudad@yahoo.com
Received : Nov 24, 2021
Accepted : Jan 13, 2022
Published : Jan 20, 2022
Archived : www.jcimcr.org
Copyright : © Foudad H (2022).
Citation: Foudad H, Bouague I, Selmani K, Trichine A. Middle - aortic syndrome with a thrombus in the renal artery. J Clin Images Med Case Rep. 2022; 3(1): 1593.
Description
A 22-year-old man with no previous medical history was admitted in our hospital for management of severe hypertension.
It’s a patient followed disorderly for high blood pressure for six months under ARB (Angiotensin II Receptor Blockers) and Calcium Antagonist with a recent elevation of his blood pressure in spite of association of a B-Adrenergic Blocker and a thiazide diuretic.
On physical examination his blood pressure measured 220/120 mmHg in both arms, with a regular pulse of 59 beats per minute. Auscultation of the abdomen revealed a murmur in the upper abdomen. Peripheral pulsations were all palpable and there was no history of abdominal pain or claudication. Serum creatinine was 67 umol/ l and Modification of Diet in Renal Disease-Glomerular Filtration Rate (MDRD-GFR) was >90 ml/ min/1.73 m2.
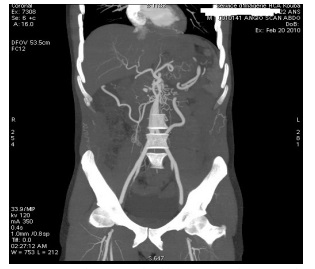
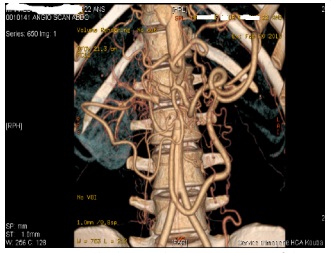
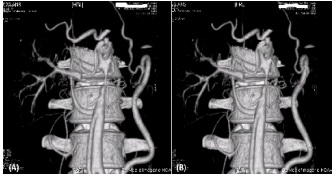
Doppler ultrasound examination demonstrated tortuosity and narrowing of the abdominal aorta with signs of the renal artery stenosis; following which he underwent Computed Tomography (CT) angiography.
Tomography (CT) angiography revealed a long segment stenosis of abdominal aorta with a thrombus in the right kidney multiple collateral vessels (Figures 1 to 4).
After discussions, a chirurgical treatment was decided; an aorto-aortic bypass from the descending thoracic aorta to the aortic bifurcation using a Dacron graft and aspiration of the thrombus in the renal artery.
The post-operative period was uneventful, his blood pressure dropped to 145/85 mmhg

References
- Rossi MA. Infrarenal aortic coarctation and diffuse hypoplasia of the aortoiliacfemoral system. Acta Cardiol. 1997; 52: 373–9.
- Cohen JR, Birnbaum E. Coarctation of the abdominal aorta. J VascSurg. 1998; 8: 160–164.
- Sen PK, Kinare SG, Engineer SD, et al. The middle aortic syndrome. Br Heart J. 1963; 25: 610–618.
- Connolly JE, Wilson SE, Lawrence PL, Fujitani RM. Middle aortic syndrome: Distal thoracic and abdominal coarctation; a disorder with multiple etiologies. J Am CollSurg. 2002; 194: 774–781.