
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Synchronous metastatic pure squamous cell carcinoma of the Gallbladder: A case report and review of literature
Ali Emadi Torghabeh1; Soudeh Arastouei2*
1 Assistant Professor of Radiation Oncology, Cancer Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
2 Resident Physician, Cancer Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
*Corresponding Author: Soudeh Arastouei
Resident Physician, Cancer Research Center, Mashhad
University of Medical Sciences, Mashhad, Iran.
Email: sou.arastouei@gmail.com
Received : Nov 25, 2021
Accepted : Jan 13, 2022
Published : Jan 20, 2022
Archived : www.jcimcr.org
Copyright : © Arastouei S (2022).
Abstract
Gallbladder cancer is an uncommon disease, comprising 1.2% of cancers in the world, with squamous cell pathology of the gallbladder being even more uncommon, making up 1-3% of those cases. When diagnosed, squamous cell carcinoma carries higher mortality when compared to all other pathologies in the gallbladder. The consensus on treatment of this cancer is inconclusive. This manuscript presents a case of a 71-year old female with squamous cell carcinoma of the gallbladder that progressed rapidly, despite resection to negative margins.
Keywords: gallbladder cancer; squamous cell carcinoma; incidental; oncology; chemotherapy.
Abbreviations: ASC: Adenosquamous Carcinoma; CEA: Carcinoembryonic antigen; CA 19-9: Carbohydrate antigen 19-9; OS: Overall Survival; PFS: Progression free survival; SCC: Squamous Cell Carcinoma.
Citation: Torghabeh AE, Arastouei S. Synchronous metastatic pure squamous cell carcinoma of the gallbladder: A case report and review of literature. J Clin Images Med Case Rep. 2022; 3(1): 1594.
Introduction
Gallbladder cancer is a rare entity; in 2018, it comprised only 1.2% of worldwide cancer diagnoses [1]. Despite its low prevalence, it is still the most common cancer of the biliary tract, and carries an OS rate of 6 months [2].
Gallbladder cancer is mostly of an adenocarcinoma pathology, while papillary, mucinous, ASC, pure squamous, and small cell subtypes have also been reported [3]. The rate of incidence of SCC of gallbladder has been reported to be 1-3% [4]. As a result of the rarity of the disease, many biological and clinicopathological features of the disease, and their relationship to their adenocarcinoma counterpart, are still unclear, and no standard treatment has been defined for this cancer. In this paper, we present a case of gallbladder cancer, found incidentally, which proved to be of pure SCC pathology.
Case presentation
A 71-year-old female presented to our hospital complaining of persistent right upper quadrant abdominal pain for 6 months. The pain had progressively worsened and she started developing icterus in the preceding month. Her past medical history included remote thyroidectomy and hemorrhoidectomy.
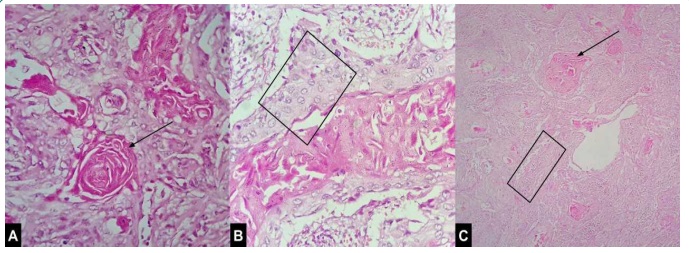
With a presumptive diagnosis of acute cholecystitis, the patient underwent a laparoscopic cholecystectomy. On gross pathological examination, the resected gallbladder had a uniformly thickened wall, with a bulky lesion in the distal end; microscopic examination demonstrated pure SCC (Figure 1). The postoperative period was uneventful and the patient’s symptoms resolved.
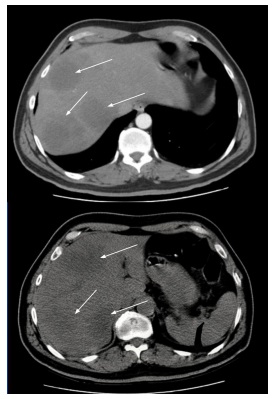
She presented to us in May 2016, three months after her surgery, completely active with an Eastern Cooperative Oncology Group performance status of 0. She was asymptomatic, with no significant abnormality on physical examination. On further evaluation, the abdominal CT scan revealed disseminated liver metastases (Figure 2). Blood tests, including complete blood count, liver function tests, and kidney function tests were all within normal limits. CEA measured at 1.2 µg/L (normal value <5 µg/L) and CA 19-9 was 15.27 U/mL (normal value <37 U/mL).
The patient was put on palliative biweekly chemotherapy regimen of gemcitabine 1,000 mg/m2 D1 and oxaliplatin 100 mg/m2 D2, which continued for 9 cycles. At the end of this course, a CT scan in September 2016, revealed a reduced number of hepatic metastases. Due to a grade 2 paresthesia and the palliative setting of treatment, the patient's chemotherapy was suspended. Two months later, the patient began experiencing abdominal pain again, and gemcitabine 1,000 mg/m2 on days 1 and 8 every three weeks was initiated, continuing for 8 cycles. The CT scan at the end of this course, in May 2017, revealed progression of disease, with increased peritoneal metastases and subcutaneous implants in the abdominal wall. At the patient's request, chemotherapy continued, but the patient deteriorated and passed away on 27th September 2017, due to complications of metastatic liver disease.
Discussion
An analysis of the National Cancer Database, during a span of 11 years, identified 1,084 cases of gallbladder SCC [5]. Out of these, only 370 cases were purely squamous. Histological analysis of the SCC tumors was noted to be just like SCC of any other site, with sheets and whorls of keratinized squamous epithelial cells, with prominent intercellular bridges and a fibrous stroma [5]. Our patient’s pathological findings also exhibited keratin pearls and intercellular bridges. In the aforementioned study’s cohort, the patients’ characteristics analysis showed a female preponderance, mostly in the older age, presenting with stage IV disease [5]. Our patient matches these characteristics, being a 71-year-old female, but differs in that she was diagnosed early, with a lesion invading the muscular layer. However, she developed liver metastases early in the course of her disease.
Jaundice has traditionally been considered a sign of advanced disease and related to poor outcome, with 44% of patients with this presentation having unresectable disease [6]. However, those presenting with jaundice alongside low CA19-9 levels have been noted to achieve more favourable survival after resection [7]. Interestingly, our patient presented with jaundice, but still resectable as the tumor only invaded the muscular layer. She also had low tumor marker levels, which may have benefited her overall survival.
Tumor extent is the most important prognostic factor, with a 5-year survival rate of 70% in tumors limited to subserosa (T2 disease), reducing to 0% when the tumor invades the serosa [2]. However, patients usually present in the advanced stage, as the symptoms may mimic those of benign diseases leading to poor detection, and anatomical features, such as the lack of a serosal layer adjacent to the liver allowing rapid invasion of adjacent organs. In spite of all her poor prognostic factors, our patient had a resectable early disease, but her survival did not equal that of her tumor extent.
The growth rate of squamous components is twice as fast as adenocarcinomatous components, and gallbladder ASC–SCC patients are often diagnosed at more advanced stages compared to pure adenocarcinoma [8]. This is likely why our patient was metastatic by the time she presented to our clinic, despite an early stage disease that was completely resected.
Due to the bulky nature of gallbladder SCC, patients can become symptomatic at an earlier stage and present with resectable disease, as was the case with our patient [4]. However, even on earlier detection, other factors, most notably growth rate of squamous components, make this a deadlier disease. This is in accordance with another study that concluded that SCC pathology has a worse prognosis, and this worse prognostic factor persisted even when compared with stage matched advanced gallbladder cancer cases [9].
Radical resection can improve survival in gallbladder cancer [6]. However, the role of radical resection after finding incidental gallbladder cancer on simple cholecystectomy is not clear. In one study, 89 incidental gallbladder cancers were found out of a total of 30,960 patients undergoing laparoscopic cholecystectomy. A significant benefit of re-resection of gallbladder bed and regional lymph nodes following incidental gallbladder cancer was observed, especially with pT2 and pT3 disease [10]. On the other hand, another study observed that in their 12 incidental gallbladder cancers, long term survival was achieved without additional resection even in pT2 and T3 disease [11]. In our case, the patient was metastatic by the time she returned for further follow up, so there was no indication for further surgical intervention.
Due to the rarity of gallbladder cancer, studies usually combine their findings with those of other biliary tract malignancies; the majority of the data is related to adenocarcinoma, with results extrapolated to SCC and ACS pathologies. The benefit of adjuvant therapy in high-risk disease, specifically those with node positive and incomplete resection, is reported in several studies, but it is not clear if radiotherapy or chemoradiotherapy is a better modality. Both the National Comprehensive Cancer Network and the European Society of Medical Oncology recommend chemoradiotherapy [12]. The most recent trial on adjuvant therapy, BILCAP, involved comparing adjuvant capecitabine to observation following radical resection. This study did not reach its primary end goal of OS, but it was significant as the treated group had longer recurrence free survival comparatively [13]. This has made capecitabine the standard of care in the adjuvant setting, surpassing the older tried gemcitabine-based regimens.
In a metastatic setting, the combined regimen of gemcitabine and cisplatin is the standard of care resulting in a PFS of 8 and OS of 11.8 months [14]. Gemcitabine alone has shown clinical benefit rates of 15-60%, while gemcitabine combined with oxaliplatin has demonstrated better response rates than single agent and a better tolerability compared to the other combinations [13]. More recent studies have tried improving the PFS in these patients, by adding nab-paclitaxel to gemcitabine-platinum combinations or using modified FOLFIRINOX (a combination regimen of folinic acid, fluorouracil, irinotecan and oxaliplatin) in this setting, both of which have shown improved results in phase II studies [14,15]. Our patient was put on gemcitabine based regimens, resulting in an OS of 19.3 months.
Conclusion
Gallbladder SCC’s rare and aggressive nature often results in poor patient outcomes. Due to a lack of specific research on this pathological subtype of gallbladder cancer, it is treated based on studies on its adenocarcinoma counterpart mostly. Studies have not yet come to a conclusion on the best adjuvant treatment modality; because of SCC’s aggressive nature, chemoradiotherapy should be considered. In a metastatic setting, while gemcitabine-based regimens are the standard of care currently, the search for a better alternative is ongoing.
Declarations
Author contributions: Both authors played a role in acquisition of the data, drafting and revising the article and have read the final version that is being submitted.
Conflicts of interest / Competing interests: None.
Grant information: The authors received no specific funding for this work.
Acknowledgements: A special thank you to Dr. Mahsa Akbari, pathologist at Omid Hospital in Mashhad, Iran, for having helped in the interpretation of pathology samples for the patient’s case.
References
- Rawla P, Sunkara T, Thandra KC, Barsouk A. Epidemiology of Gallbladder Cancer. Clinical and Experimental Hepatology. 2019; 5: 93-102.
- Shaffer E and Hundal R. Gallbladder cancer: Epidemiology and outcome. Clinical Epidemiology. 2014; 6: 99-109.
- Samuel S, Mukherjee S, Ammannagari N, Pokuri VK, Kuvshinoff B, Groman A, et al. Clinicopathological characteristics and outcomes of rare histologic subtypes of gallbladder cancer over two decades: A population-based study. PLoS One. 2018; 13: e0198809.
- Perisetti A, Raghavapuram S, Tharian B, Warraich I, Hardwicke F, Rahman R, et al. Pure squamous cell carcinoma of the gallbladder masquerading as a hepatic mass. Cureus. 10: e201.
- Ayabe RI, Wach MM, Ruff SM, Diggs LP, Martin SP, Wiemken T, et al. Gallbladder squamous cell carcinoma: An analysis of 1084 cases from the National Cancer Database. J Surg Oncol. 2020; 122: 716-722.
- Misra S, Chaturvedi A, Misra NC, Sharma ID. Carcinoma of the gallbladder. Lancet Oncol. 2003; 4: 167-176.
- Tran TB, Norton JA, Ethun CG, Pawlik TM, Buettner S, Schmidt C, et al. Gallbladder cancer presenting with jaundice: Uniformly fatal or still potentially curable? Journal of Gastrointestinal Surgery. 2017; 21: 1245-1253.
- Charbit A, Malaise EP, Tubiana M. Relation between the pathological nature and the growth rate of human tumors. Eur J Cancer. 1971; 7: 307-315.
- Roa JC, Tapia O, Cakir A, Basturk O, Dursun N, Akdemir D, et al. Squamous cell and adenosquamous carcinomas of the gallbladder: Clinicopathological analysis of 34 cases identified in 606 carcinomas. Mod Pathol 2011 248. 2011; 24: 1069-1078.
- Glauser PM, Strub D, Käser SA, Mattiello D, Rieben F, et al. Incidence, management, and outcome of incidental gallbladder carcinoma: Analysis of the database of the Swiss Association of Laparoscopic and thoracoscopic surgery. Surgical Endoscopy. 2010; 24: 2281-2286.
- Sugiyama T, Makino K, Fukui Y, Kinoshita H, Miki A, Uchida S, et al. Long term outcomes of incidental gallbladder carcinoma without additional resection: A single institution experiment. Molecular and Clinical Oncology. 2020; 13: 216-220.
- Kanthan R, Senger JL, Ahmed S, Kanthan SC. Gallbladder cancer in the 21st century. J Oncol. 2015; 2015: 967472.
- Primrose JN, Fox RP, Palmer DH, Malik HZ, Prasad R, Mirza D, et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019; 20: 663-673.
- Shroff RT, Javle MM, Xiao L, Kaseb AO, Varadhachary GR, Wolff RA, et al. Gemcitabine, Cisplatin, and nab-Paclitaxel for the Treatment of Advanced Biliary Tract Cancers: A Phase 2 Clinical Trial. JAMA Oncol. 2019; 5: 824-830.
- Cui XY, Li XC, Cui JJ, Wu XS, Zou L, Song XL, et al. Modified folfirinox for unresectable locally advanced or metastatic gallbladder cancer, a comparison with GEMOX regimen. Hepatobiliary Surgery and Nutrition. 2021; 10: 498-506.