
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Retained gallstones: A forgotten complication after laparoscopic cholecystectomy
Manar Shmais, MD1; Tarek Nammour, MD1; Fady Daniel, MD2*
1 Fellow, Division of Gastroenterology, American University of Beirut, Lebanon.
2 Associate Professor of Medicine, Division of Gastroenterology, American University of Beirut, Lebanon.
*Corresponding Author: Fady Daniel, MD
Associate Professor of Medicine, Division of Gastroenterology, American University of Beirut, Lebanon.
Email: fd21@aub.edu.lb
Received : Nov 25, 2021
Accepted : Jan 13, 2022
Published : Jan 20, 2022
Archived : www.jcimcr.org
Copyright : © Daniel F (2022).
Keywords: cholecystectomy; gallstones; surgical complications.
Citation: Shmais MA, Nammour T, Daniel F. Retained gallstones: A forgotten complication after laparoscopic cholecystectomy. J Clin Images Med Case Rep. 2022; 3(1): 1596.
Clinical image description
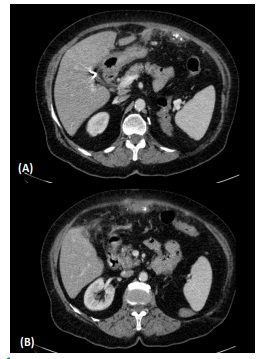
A 68-year-old woman with history of Laparoscopic Cholecystectomy (LC) for symptomatic gallstones 1 month ago, presented to the emergency department for mid abdominal pain since surgery. The pain is severe, continuous and unrelated to food. Her past medical history is significant for Diabetes Mellitus Type 2. On physical examination, she had localized abdominal tenderness and guarding at two surgical sites with skin induration. Laboratory studies were significant for leukocytosis (WBC 15,200) and elevated C- Reactive Protein of 150 mg/L. A contrast enhanced abdominal and pelvic CT scan showed postsurgical changes in the anterior abdominal wall and peritoneal calcification in the anterior aspect of the peritoneal cavity with associated fat stranding (Figure A and B).
Retained gallstones, also called slipped or dropped gallstones, are relatively common during laparoscopic cholecystectomy with reported incidence of 7-30% as a result of gallbladder perforation during surgical dissection or extraction. However, these stones rarely become symptomatic and only lead to adverse events in 0.08-0.3% [1]. Retained GS can disperse in the intraperitoneal space, subhepatic space, port sites, retroperitoneum or dependent areas such as the pelvis or pass through the diaphragm [2]. The most common complication is abscess formation which can present with a median interval of 5 months after cholecystectomy but latencies of up to 20 years has been reported [1]. The diagnosis of retained gallstones is challenging. Both radiolucent and radiopaque gallstones may be undetected at standard imaging. CT and MRI abdomen may be helpful in detecting retained GS and inflammatory changes/abscess. The definitive treatment of abscess associated with retained GS is removal of these stones to prevent recurrent abscess formation [3]. Studies have shown that retained GS at trocar sites may cause higher incidence of infectious complications. Routine use of bags during the retrieval of gallbladders seems helpful to avoid this complication [4].
Author’s contributions
M Shmais: Acquisition of data; analysis and interpretation of data; drafting of the manuscript. T Nammour: Drafting of the manuscript and critical review of the manuscript. F Daniel: Study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; and critical review of the manuscript.
References
- Ramamurthy NK, Rudralingam V, Martin DF, Galloway SW, Sukumar SA. Out of sight but kept in mind: Complications and imitations of dropped gallstones. AJR Am J Roentgenol. 2013; 200: 1244-1253.
- Jabbari Nooghabi A, Hassanpour M, Jangjoo A. Consequences of Lost Gallstones During Laparoscopic Cholecystectomy: A Review Article. Surg Laparosc Endosc Percutan Tech. 2016; 26: 183-192.
- Nayak L, Menias CO, Gayer G. Dropped gallstones: spectrum of imaging findings, complications and diagnostic pitfalls. Br J Radiol. 2013; 86: 20120588.
- Demirbas BT, Gulluoglu BM, Aktan AO. Retained abdominal gallstones after laparoscopic cholecystectomy: A systematic review. Surg Laparosc Endosc Percutan Tech. 2015; 25: 97-99.