
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Membranous web in aqueduct of sylvius on FIESTA-C and 3D-BRAVO MR sequence in an adult
Neetu Sinha*; Ruchi Gupta; Waghmare Vaibhav
Department of Radiodiagnosis, Indira Gandhi Institute of Medical Sciences, Patna, India.
*Corresponding Author: Neetu Sinha
Department of Radiodiagnosis , Indira Gandhi
Institute of Medical Sciences, Patna, India.
Email: dr.neetu.sinha@gmail.com
Received : Nov 02, 2021
Accepted : Jan 14, 2022
Published : Jan 21, 2022
Archived : www.jcimcr.org
Copyright : © Sinha N (2022).
Abstract
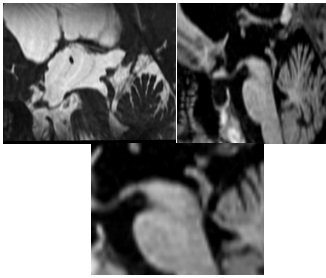
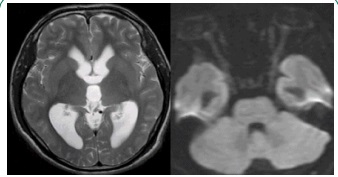
We present a case of 38-year-old man who presented with persisted mild headache and occasional vision loss for four and half years. MRI of brain revealed tri-ventricular dilatation with uninvolved fourth ventricle. On the FIESTA-C and 3D-BRAVO MR sequences, two thin membranous webs were seen in the distal part of the aqueduct of sylvius. At present, the FIESTA sequence is the preferred imaging method for the aqueduct web/diaphragm, but both FIESTA and 3DBRAVO can show the web in aqueduct as well.
Citation: Sinha N, Gupta R, Vaibhav W. Membranous web in aqueduct of sylviuson FIESTA-C and 3D-BRAVO MR sequence in an adult. J Clin Images Med Case Rep. 2022; 3(1): 1600.
Description
A 38-year-old man has had mild generalized headache for four and a half years. Headache occurred intermittently on most days and persisted for few hours. It was associated with occasional transient loss of vision and exacerbated by cough. No significant increase in severity over time was observed. The patient did not have any hydrocephalus related complaints in childhood. Brain MRI performed on the 1.5T GE system with additional FIESTA-C and 3D-BRAVO sequences showed moderate dilation of the bilateral and third ventricles without periventricular interstitial oedema, and the fourth ventricle was normal. In the midsagittal FIESTA-C and 3D-BRAVO sequences, two thin membranous webs were seen in the lower third of the aqueduct. The proximal aqueduct was dilated due to web in the distal lumen.
Congenital webs are an important cause of idiopathic adult onset aqueductal stenosis. Membranous web arises from gliosis forming a septum of glial cells across the aqueduct [1]. These webs are easily amenable to treatment by endoscopic ventriculostomy [2]. In this case, both BRAVO and FIESTA -C sequences accurately demonstrated the anatomic details of the aqueduct. However, on FIESTA-C sequence, the thinner membranes or webs are displayed best against the bright background of CSF. FIESTA - C is an improved fast 3D balanced steady-state gradient echo sequence that provides high-resolution images for accurately visualising the fine luminal details of the aqueduct [3]. Since BRAVO is a T1 GRE (gradient echo) sequence and CSF signal is nulled, it fails to provide the same image contrast between the web and CSF in aqueduct as seen on the FIESTA sequence. But because of its being ultra-fast high-resolution 3D sequence, it is sufficient in the absence of FIESTA sequence.
References
- Sainte Rose, Christian. & Cinalli, G & Maixner, W. J. Pediatric hydrocephalus. Milano London: Springer. 2004.
- Jones RF, Stening WA, Brydon M. Endoscopic third ventriculostomy. Neurosurgery. 1990; 26: 86-91. discussion 91-92.
- Algin O, Hakyemez B, Parlak M. Phase-contrast MRI and 3D-CISS versus contrast-enhanced MR cisternography on the evaluation of the aqueductal stenosis. Neuroradiology. 2010; 52: 99-108.