
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Anaesthetic management of fetal congenital diaphragmatic hernia by EXIT: A case report
Xiaoli Liang; Danyong Liu; Yajing Gao; Yuci Xiao; Xiaolei Huang; Yuantao Li*
Department of Anesthesiology, Shenzhen Maternity and Child Healthcare Hospital, Southern Medical University, Shenzhen, Guangdong, China.
*Corresponding Author: Yuantao Li
Department of Anesthesiology, Shenzhen Maternity
and Child Healthcare Hospital, Southern Medical
University, Shenzhen 518028, Guangdong, China.
Email: szmchlyt@smu.edu.cn
Received : Dec 24, 2021
Accepted : Jan 14, 2022
Published : Jan 21, 2022
Archived : www.jcimcr.org
Copyright : © Li Y (2022).
Abstract
We present a case of congenital diaphragmatic hernia (CDH) diagnosed in the second trimester of pregnancy, with most of the stomach and part of the liver occupying half of the left hemithorax. Severe pulmonary hypoplasia is associated with reduced survival in patients with CDH. The pregnant woman was treated with Exutero intrapartum treatment (EXIT) at 38 weeks of gestation. Open fetal and EXIT procedures require maternal general anesthesia with volatile anesthetic and other medications to maintain uterine relaxation. Through this case, our team summarized some experience in perioperative period anesthetic management of EXIT.
Keywords: CDH; EXIT procedure; fetal surgery; maternal anaesthesia.
Citation: Liang X, Liu D, Gao Y, Xiao Y, Li Y, et al. Anaesthetic management of fetal congenital diaphragmatic hernia by EXIT: A case report. J Clin Images Med Case Rep. 2022; 3(1): 1603.
Introduction
Congenital diaphragmatic hernia (CDH), which occurs in about 1 in 3300 live births, is a congenital defect in the diaphragm that allows herniation of abdominal viscera into the thorax [1]. With the development of technological advances in prenatal fetal imaging and genetic diagnosis, obstetricians have a better understanding of the disease progression and pathophysiology of several fetal anomalies. Ex-utero intrapartum treatment (EXIT) is a type of fetal surgery, which refers to the technique of performing surgical treatment on the fetus under the condition of continuous umbilical cord to maintain the fetus-placental circulation during cesarean section [2].
Perform anesthesia for EXIT is undoubtedly a challenge for anesthesiologists because it involves both maternal and fetal anesthesia. Anaesthetic care needs to take into account normal maternal and neonatal physiology, the pathology leading to the procedure, the surgery and how these interact to impact on the health of the mother and fetus [3]. For success, meticulous planning is required, with multiple teams and disciplines involved throughout the peri-operative journey
Case report
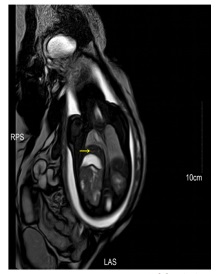
A 29-year-old pregnant woman was diagnosed fetal malformation in the second trimester pregnancy in another hospital. At 36 weeks of gestation, the three-dimensional ultrasound in our institution showed that the fetal thoracic cavity sound image changes, considering the left diaphragm eventration or diaphragmatic hernia. The parturient was admitted to our institution for delivery at 37 weeks and 6 days of gestation. After admission, the parturient’s vital signs were stable, and the examination of various organs and systems showed no abnormalities. Pelvic placenta - fetal chest MRI before surgery, The results suggest that most of the stomach and part of the liver occupying half of the left hemithorax, which shifted the cardiothymic structures to the middle (Figure 1).
Obstetricians, neonatologists, and pediatric surgeons have a preoperative consultation, considering that fetal malformations appear earlier and the left lung of the fetus may be compressed for a long time, which may lead to fetal lung dysplasia and respiratory insufficiency. Once the fetus was born, fetal spontaneous breathing is established after the umbilical cord clamping, abnormal left lung function may endanger the life of the neonate. Surgical specialists recommend EXIT for the fetus, which can be surgically repaired using placental circulation when the fetus has not yet established spontaneous breathing, thus improving the probability of neonatal survival.
The procedure of surgery and anesthesia
After the parturient entered the operating room at 30°C, standard monitoring was carried out (HR 90 bpm, BP 108/57 mmHg, SpO2 99%, FHR 143 bpm), and open a peripheral venous access (liquid was heated at 37°C), ritodrine was injected intravenously at a rate of 0.1 mg/min. Combined intravenous inhalational anesthesia was scheduled, general anesthesia was induced by intravenous injection of propofol 150 mg and rocuronium 50 mg and sufentanil 15 µg, tracheal intubation, left radial artery and right subclavian vein puncture catheterization were performed, then proceed temperature and depth of anesthesia monitoring, catheterization. Intravenous injection of rocuronium 25 mg and sufentanil 20 μg before the operation. Inhalation a high dose of desflurane to achieve maternal endexpirative desflurane concentration of 2-3 MAC (minimum alveolar concentration), compound intravenously pumping of propofol 4-5 mg/(kg.h) and remifentanil 0.2-0.4 µg/(kg.min) maintain anesthesia before cutting the umbilical cord.
Narcotrend anesthesia depth monitoring was maintained at the level of E0 to E1, maternal blood pressure fluctuation was 120-140/60-70 mmHg, HR fluctuates within 70-80 bpm (Phenylephrine was injected intravenously at a rate of 0.5-2 μg/(kg.min), if necessary, intravenous bolus a single dose of ephedrine 5 mg). After removing the fetus from the maternal uterus, the umbilical cord was kept, and the fetus was transferred to another sterile operating table near the incision of the mother’s uterus, monitor the fetal anal temperature, heart rate and SpO2 . The fetus was placed in the right decubitus position, and the pediatric surgeon opened the chest through the 5th and 6th front axillary lines of the left thoracic cavity, the surgeon found the fetal left side diaphragm was weak, protruding into the thoracic cavity, and the diaphragm protruding to the sixth intercostal space, compressing the left lung, there was no obvious air leakage and damage to the left lung. During the fetal surgery, the FHR fluctuated at 140-160 beats/min, and SpO2 kept in 40%-50%. Cover the uterine incision, umbilical cord, and fetal exposure with 40o C saline wetted gauze and keep the umbilical cord from twisting, squeezing, folding and stretching. In this case, the fetus was performed a left diaphragm plication. After the EXIT, the fetus was immediately intubated and connected to a ventilator to control breathing and transferred to the NICU). Litodrine and desflurane were stopped immediately after the umbilical cord was cut off, and 20 u of oxytocin was injected into the mother’s vein and uterus respectively, propofol and remifentanil were to maintain the anesthesia. At the end of the operation, carboprost 1 mg was placed in the vagina, bilateral TAPB and PCIA was performed, a high-flow oxygen was used for replacement with residual desflurane in the lungs. The mother was observed in the resuscitation room for 1 hour after she was wake up from anesthesia, and then returned to the ward smoothly. The entire procedure lasted 1 hour and 55 minutes. The fetal left diaphragmatic plication lasted 25 minutes, fetal bleeding volume was 2 ml, maternal bleeding volume was 300 ml, urine volume was 400 ml, and the infusion volume was 2000 ml.
Maternal and neonatal outcome
The puerperal woman wound healed well without postpartum bleeding or infection, and was discharged 7 days after surgery. The newborn boy, weighing 3240 g, did not breathe spontaneously after umbilical cord cutting, had ruddyfaced face and flabby limbs. Apgar score was 4 at 1 and 5 minutes after birth. After endotracheal intubation, he received ventilator controlled ventilation, and immediately underwent bedside chest X-ray examination, which indicated that the left lung was transparent and normal without substantial lesions (Figure 2). The newborn was transferred to NICU after birth, and the ventilator was taken off 10 days after surgery. His total hospital stay was 23 days, and chest X-ray reexamination before discharge showed that both lungs were transparency and normal (Figure 3). All developmental indicators were normal during 1-year follow-up.


Discussion
CDH is an abnormal elevation of the diaphragm caused by diaphragmatic hypoplasia or absence of diaphragmatic nerve [4]. In severe cases, the diaphragm is compressed against the chest cavity, affecting respiratory function and the growth of fetus. EXIT is usually performed when the parturient is close to or has a full-term pregnancy [5], the fetus is delivered from the maternal immediately after the operation. This case is an indication for the implementation of EXIT.
During cesarean section, the anesthesia for the fetus to perform EXIT procedure have to meet the anesthesia needs of both the maternal and the fetal, majority of EXIT procedures are performed under general anaesthesia using high concentrations of volatile anaesthetics combined with intravenous anesthetics to make the maternal reach a deep anesthesia and at the time of fetal surgery to facilitate uterine relaxation [6,7]. One of the goals of maternal anesthesia is to optimize placental perfusion by maintaining maternal blood pressure and uterine relaxation. When the fetus reaches enough depth of anesthesia, the mother is often in a state of deep anesthesia [8]. High concentration of inhalation anesthesia can cause maternal hypotension by inhibiting maternal circulation, which is harmful to both the mother and the fetus. Therefore, vasoactive medications will be necessary to maintain blood pressure. Arterial blood pressure monitoring is preferable for titration of vasoactive medications [7]. Also the integrity of the uterine-placental connection should be ensured to prevent compression of the umbilical cord and placenta; On the other hand, high-concentration inhalation anesthetics can inhibit uterine contractions, in order to reduce the use of inhaled anesthetics, a combination of uterine contractions inhibitors such as the β2 agonist such as ritodrine, magnesium sulfate, and nitroglycerin keeps the uterus in a good state of relaxation [9]. In this case, the maternal inhalation of desflurane combined with propofol and remifentanil during fetal EXIT enabled the fetus to successfully complete the operation with the characteristics of rapid induction and early awakening. Inhalation of desflurane combined with intravenous infusion of ritodrine to achieve Satisfied uterine relaxation, intravenous pump injection of phenylephrine in order to maintain stable maternal hemodynamics and good placental perfusion.
Muscle relaxants rarely pass through the placental barrier. it can be injected intramuscular or umbilical vein to prevent fetal movement, the dose of vecuronium is 0.3 mg/kg intramuscular injection, 0.1-0.25 mg/kg intravenously [10]. Normal fetal arterial oxygen saturation is 40%-70% [10]. Rectal temperature, FHR and SpO2 should be monitored during EXIT procedure, if the fetus has a long-term Bradycardia and decreased oxygen saturation (FHR<120 beats/min, SpO2 <40%), placental dissection, umbilical cord compression or torsion, maternal hypotension, fetal hypothermia and other causes [10] should be quickly considered and corrected, and intraoperative ultrasound evaluation of the fetus If necessary, atropine and epinephrine can be injected intramuscularly or intravenously through the fetus.
After the EXIT, neonatal pediatrician will intubate the fetus, and the inhalation anesthetic should be stopped immediately after umbilicus clamping. At this time, the key of anesthetic management is to reverse uterine relaxation as soon as possible [9]. Oxytocin, ergometrine and hemabate can be used to enhance uterine contraction, promote the separation of placenta from the maternal and reduce maternal bleeding. Fetal body temperature cannot be self-regulated, it temperature depends on maternal body temperature. General anesthesia induction, surgical exposure and hysterectomy can significantly reduce the fetal body temperature [10]. In this case, the temperature was adjusted to 30°C in the operating room, the maternal infusion was heated to 37°C in the whole process, and 40°C saline wetted gauze was frequently changed to cover the uterine incision, umbilical cord and fetal unoperated part. The maternal and fetal body temperatures were normal during the operation.
Conclusion
In summary, the key points of anesthetic management of EXIT for the fetus during cesarean section include the following: 1) Ensuring sufficient uterine relaxation during fetal surgery; 2) Maintaining uterine placenta circulation, stabilizing maternal hemodynamics; 3) Ensuring uterine cavity capacity, and keeping maternal fetus warm throughout the operation; 4)After umbilical cord clamping, uterine relaxation should be reversed as soon as possible to promote uterine contraction and avoid excessive bleeding due to lack of contraction [3].
Declarations
Competing interests: The authors have declared that no competing interest exists.
Acknowledgment: The authors’ research was supported by Special Fund for Young and Middle-aged Medical Research of China Foundation for International (No. Z-2018-35-1903).
References
- Puligandla PS, Skarsgard ED, Offringa M, et al. Diagnosis and management of congenital diaphragmatic hernia: a clinical practice guideline. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne. 2018; 190(4): E103-e112.
- Abraham RJ, Sau A, Maxwell D. A review of the EXIT (Ex utero Intrapartum Treatment) procedure. Journal of obstetrics and gynaecology: The journal of the Institute of Obstetrics and Gynaecology. 2010; 30(1): 1-5.
- Dick JR, Wimalasundera R, Nandi R. Maternal and fetal anaesthesia for fetal surgery. Anaesthesia. 2021; 76 Suppl 4: 63- 68.
- Patra C, Singh NG, Manjunatha N, Bhatt A. Anaesthetic management of an infant posted for ventricular septal defect closure with right-sided eventration of diaphragm. Indian journal of anaesthesia. 2018; 62(2): 136-138.
- Chatterjee D, Arendt KW, Moldenhauer JS, et al. Anesthesia for Maternal-Fetal Interventions: A Consensus Statement From the American Society of Anesthesiologists Committees on Obstetric and Pediatric Anesthesiology and the North American Fetal Therapy Network. Anesthesia and analgesia 2021; 132(4): 1164- 1173.
- Kumar K, Miron C, Singh SI. Maternal anesthesia for EXIT procedure: A systematic review of literature. Journal of anaesthesiology, clinical pharmacology. 2019; 35(1): 19-24.
- Kodali BS, Bharadwaj S. Foetal surgery: Anaesthetic implications and strategic management. Indian journal of anaesthesia 2018; 62(9): 717-723.
- Joshi H, Packiasabapathy S. Anesthetic Management Of Ex Utero Intrapartum Treatment (EXIT) And Fetal Surgery. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC. 2021.
- Lin EE, Moldenhauer JS, Tran KM, Cohen DE, Adzick NS. Anesthetic Management of 65 Cases of Ex Utero Intrapartum Therapy: A 13-Year Single-Center Experience. Anesthesia and analgesia 2016; 123(2): 411-417.
- Ferschl MB, Rollins MD. Anesthesia for fetal surgery and other fetal therapies. In: Eriksson L, Gropper MA, eds. Miller’s Anesthesia, 9th Edition. hiladelphia, PA: Mosby Elsevier. 2020; 2042-2070