
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Acute pancreatitis associated with gangrenous cholecystitis in the absence of definitive laboratory or imaging evidence: Case report and literature review
Hongxin Kang1; Hang Su2; Meihua Wan1*
1 Department of Integrative Medicine, West China Hospital, Sichuan University, Chengdu, Sichuan Province, China.
2 Health Management Center, West China Hospital, Sichuan University, Chengdu, Sichuan Province, China.
*Corresponding Author: Meihua Wan
Department of Integrative Medicine, West China
Hospital, Sichuan University, #37 Guoxue Alley,
Chengdu 610000, Sichuan Province, China.
Email: wanmh@scu.edu.cn
Received : Dec 24, 2021
Accepted : Jan 17, 2022
Published : Jan 24, 2022
Archived : www.jcimcr.org
Copyright : © Wan M (2022).
Abstract
Gangrenous cholecystitis (GC) is the most severe form of cholecystitis and is associated with acute pancreatitis. Once GC diagnosis is established, urgent cholecystectomy is recommended. The preoperative diagnosis is challenging, and clinical judgment can be critical. We report a case of GC with acute pancreatitis diagnosed in the absence of definite laboratory or imaging evidence.
Keywords: gangrenous cholecystitis; acute pancreatitis; diagnosis; clinical judgment.
Abbreviations: GC: Gangrenous cholecystitis; CT: computed tomography
Citation: Kang H, Su H, Wan M. Acute pancreatitis associated with gangrenous cholecystitis in the absence of definitive laboratory or imaging evidence: Case report and literature review. J Clin Images Med Case Rep. 2022; 3(1): 1605.
Introduction
Gangrenous cholecystitis (GC) is a particularly severe form of acute cholecystitis [1], a potentially life-threatening inflammation of the gallbladder that is sometimes associated with acute pancreatitis [2]. GC diagnosis is based on clinical symptoms, laboratory parameters and imaging findings [3], and once established, immediate cholecystectomy is recommended [4] due to its potential ability to improve the clinical outcomes of GC patients [5]. Preoperative GC diagnosis is often very challenging [6]; however, clinical judgment and experience can be critical for accurate diagnosis.
Case presentation
A 63-year-old man presented with severe right upper abdominal pain after 2 days of excessive food intake. He complained of nausea and bilious vomiting and was admitted via the emergency department, where ultrasonography detected gallstones within an enlarged gallbladder and an irregular pancreas. Relevant laboratory findings on admission were as follows: serum amylase 60 IU/L; white blood cell count 6.5 X 109 /L; red blood cell count 3.31 X 1012/L; hemoglobin 103 g/L; platelet count 171 X 109 /L; total bilirubin 19.9 µmol/L; direct bilirubin 11.0 µmol/L; indirect bilirubin 8.9 µmol/L; alanine transaminase 103 IU/L; aspartate transaminase 91 IU/L; lactate dehydrogenase 614 U/L; blood urea nitrogen 3.07 mmol/L; serum creatinine 65.0 mmol/L; serum potassium 3.87 mmol/L; serum calcium 2.03 mmol/L; fasting blood glucose 6.12 mmol/L; C-reactive protein 101 mg/L; and procalcitonin 0.34 mg/mL. Physical examination revealed reduced breath sounds in both lower lung fields and a non-distended soft abdomen with marked tenderness in the right upper quadrant. There was no palpable organomegaly and no clinical evidence of ascites. The remainder of the examination was unremarkable. Observation parameters were as follows: core temperature 37.3o C; respiratory rate 22 breaths per minute; heart rate of 72 beats per minute; blood pressure 107/71 mmHg. Based on the above findings, a preliminary diagnosis of acute pancreatitis and cholecystitis secondary to gallstones was made. Treatments consisting of fasting, fluid resuscitation, antibiotics and proton pump inhibitors were initiated.
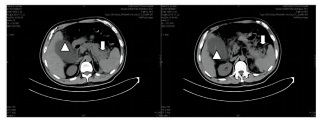
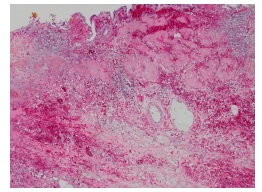
Over the course of the next 48 hours, however, the abdominal pain worsened significantly, and the patient developed peritonitis in the right upper quadrant. Due to unexplained deterioration, a computed tomography (CT) was ordered but performed without contrast enhancement due to the patient’s previously noted contrast allergy. This revealed pancreatic edema with extrapancreatic collections, pleural effusions and gallstones within a thick-walled, distended gallbladder (Figure 1). These clinical findings appeared out of proportion with what could be attributed to pancreatitis alone; therefore, a decision for urgent surgical intervention was made on day 3 of admission. Intra-operative findings were a diffusely reddish-black gallbladder containing multiple gallstones and mucosal necrosis. The gallbladder measured 9.5 X 5.0 X 3.0 cm with a wall thickness of 0.2-0.5 cm. Histological examination identified features consistent with GC (Figure 2). Abdominal pain was rapidly relieved following surgery, and the patient was discharged home on day 11 after achieving a complete recovery.
Discussion
Acute pancreatitis is an inflammatory disease where there is autodigestion of the pancreas by prematurely activated enzymes, and may lead to a systemic inflammatory response, distal organ failure and sepsis [7]. The most common etiology of acute pancreatitis is of biliary origin, and acute cholecystitis is also often reported as an association [8,9], but GC is rarely associated with acute pancreatitis [2]. As one of the few studies, Chen et al [2] presented 10 GC patients with acute pancreatitis and compared their clinical outcomes to those of patients who did not have GC. They found that GC patients had significantly higher rates of multiple organ dysfunction syndrome, septic shock and death, highlighting the importance of early GC diagnosis and management of GC in the context of acute pancreatitis.
Nevertheless, making a preoperative diagnosis of GC in the setting of acute pancreatitis is difficult, as there are no truly specific clinical or laboratory markers, and pancreatitis itself can often account for encountered abnormalities. Imaging modalities such as ultrasonography, CT, magnetic resonance imaging and radioisotope scanning can help differentiate between diagnoses [10], with contrast-enhanced CT being of great value in diagnosis. The CT findings in GC are those of a tensely distended gallbladder, with or without mucosal discontinuity or irregular enhancement of the gallbladder wall, and pericholecystic fluid [11, 12]. The presence of gallstones in the gallbladder neck or cystic duct may also be suggestive of GC [1].
Our case highlights the fact that one needs to constantly revise a working diagnosis in light of either new clinical and/ or radiological evidence or, indeed, in situations where there is an unexplained clinical course, or deterioration despite optimal treatment. As in our case, it is occasionally impossible to obtain optimal imaging, and in such cases, the importance of a good history and examination cannot be stressed enough, and the decision to operate may still have to be made in the absence of radiological proof.
Conclusion
GC is infrequently associated with acute pancreatitis; in addition, making a preoperative diagnosis of GC in the setting of acute pancreatitis is very challenging. It is particularly critical for clinicians to carefully and timely analyze and judge patients’ symptoms and examinations under these circumstances.
Declarations
Authors’ contributions: Hongxin Kang and Hang Su wrote the manuscript; Meihua Wan provided substantive intellectual contributions and improvements. All authors read and approved the final manuscript.
Conflicts of interest: The authors declare no conflict of interest.
Grant information: This study has no financial assistance from any private or governmental organizations or agencies.
Consent: Written informed consent was obtained from the patient for the publication of both the case report and accompanying images.
References
- Sureka B, Jha S, Rodha MS, et al. Combined hyperdense gallbladder wall-lumen sign: new computed tomography sign in acute gangrenous cholecystitis. Pol J Radiol. 2020; 85: e183-e187.
- Chen EZ, Huang J, Xu ZW, Fei J, Mao EQ, Zhang SD. Clinical features and outcomes of patients with severe acute pancreatitis complicated with gangrenous cholecystitis. Hepatobiliary Pancreat Dis Int. 2013; 12(3): 317-23.
- Safa R, Berbari I, Hage S, Dagher GA. Atypical presentation of gangrenous cholecystitis: A case series. Am J Emerg Med. 2018; 36(11): 2135.e1-2135.e5.
- Qutbi M, Ahmadi R. Pericholecystic Rim Sign and Gallbladder Nonvisualization Indicating Acute Gangrenous Cholecystitis on 99mTc-MIBI Myocardial Perfusion SPECT. Clin Nucl Med. 2019; 44(4): 339-340.
- Goh S, Chia C, Ong JW, et al. Improved outcomes for index cholecystectomy for acute cholecystitis following a dedicated emergency surgery and trauma service (ESAT). Eur J Trauma Emerg Surg. 2020 .
- Andalib I, Kats D, Tyberg A, et al. Hybrid management of perforated gangrenous gallbladder. Endoscopy. 2019; 51(12): E370-E371.
- Garg PK, Singh VP. Organ Failure Due to Systemic Injury in Acute Pancreatitis. Gastroenterology. 2019; 156(7): 2008-2023.
- Dai W, Zhao Y, Du GL, Zhang RP. Comparison of early and delayed cholecystectomy for biliary pancreatitis: A meta-analysis. Surgeon. 2020.
- Maldonado I, Shetty A, Estay MC, et al. Acute Pancreatitis Imaging in MDCT: State of the Art of Usual and Unusual Local Complications. 2012 Atlanta Classification Revisited. Curr Probl Diagn Radiol. 2020.
- Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018; 25(1): 41-54.
- Singh AK, Sagar P. Gangrenous cholecystitis: prediction with CT imaging. Abdom Imaging. 2005; 30(2): 218-21.
- Sureka B, Rastogi A, Mukund A, Thapar S, Bhadoria AS, Chattopadhyay TK. Gangrenous cholecystitis: Analysis of imaging findings in histopathologically confirmed cases. Indian J Radiol Imaging. 2018; 28(1): 49-54.