
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
New right bundle branch block after selective HIS bundle pacing, Two methods for correction
Mohamed Sharief1; G André Ng2,3; Mokhtar Ibrahim3,4*
1 Mansoura University hospitals, Egypt.
2 Department of Cardiovascular Sciences, University of Leicester, NIHR Leicester Biomedical Research Centre, Glenfield Hospital, Groby Road, Leicester, LE3 9QP, UK.
3 University Hospitals of Leicester NHS Trust, Glenfield Hospital, Groby Road, Leicester, LE3 9QP, UK.
4 Ain Shams University, Egypt.
*Corresponding Author: Mokhtar Ibrahim
Department of Cardiovascular Sciences, University of
Leicester, NIHR Leicester Biomedical Research,
Centre, Glenfield Hospital, Leicester, United Kingdom.
Email: mokhtar.ibrahim@uhl-tr.nhs.uk
Received : Nov 26, 2021
Accepted : Jan 17, 2022
Published : Jan 24, 2022
Archived : www.jcimcr.org
Copyright : © Ibrahim M (2022).
Abstract
HIS Bundle Pacing (HBP) is considered the most physiologic pacing technique as it generates a physiological activation of both ventricles through synchronous ventricular depolarization of His bundle– Purkinje conduction system. Permanent HBP and Atrioventricular Node (AVN) ablation in patients with heart failure and atrial fibrillation were found to have an improvement in cardiac function and reduction of left ventricular dimensions [1].
We present case of paroxysmal atrial fibrillation and atypical atrial flutter that underwent HBP and AVN ablation. The patient developed a Right Bundle Branch Block (RBBB) following his AVN ablation with widening of QRS duration to 148 msec. We managed to correct this and restore a narrow QRS by two different mechanisms:
1. Programming the Interventricular (VV) delay to 20 msec (His pacing first followed by septal RV pacing through a back-up lead, 2. Unipolar pacing of the HIS lead with different configuration. By both methods, QRS duration was reduced to 108-110 msec with restoration of physiologic biventricular pacing. To the best of our knowledge, this has not been reported before.
Keywords: atrial fibrillation; his bundle pacing; ablate; pace.
Citation: Sharief M, André Ng G, Ibrahim M. New right bundle branch block after selective HIS bundle pacing, Two methods for correction. J Clin Images Med Case Rep. 2022; 3(1): 1607.
Introduction
His bundle pacing (HBP) as a method of Cardiac Resynchronization Therapy (CRT) can generate physiological activation of both ventricles through synchronous ventricular depolarization of bundle–Purkinje conduction system. Permanent HBP and Atrioventricular Node (AVN) ablation in patients with heart failure and atrial fibrillation were found to have an improvement in cardiac function and reduction of left ventricular dimensions [1].
Permanent HBP and AVN ablation significantly improved echocardiographic measurements and New York Heart Association classification (NYHA) and reduced diuretics use for heart failure management in atrial fibrillation patients with narrow QRS who suffered from heart failure with preserved or reduced ejection fraction [2].
The present case study aims to report a case of paroxysmal atrial fibrillation and atypical atrial flutter that underwent HBP then developed a Right Bundle Branch Block (RBBB).
Case report
A 68-year-old gentleman has been suffering from paroxysmal Atrial Fibrillation (AF) and atypical atrial flutter. He underwent three catheter ablation procedures in the past few years. He presented with recurrent symptomatic atrial tachyarrhythmia. He deemed not suitable for a redo procedure, rather, he opted for Atrioventricular Node (AVN) ablation and a pacemaker implant.
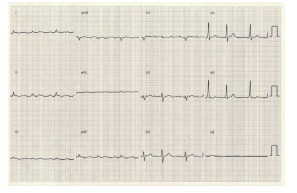
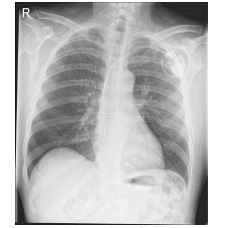
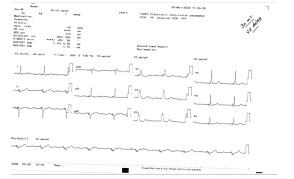
Due to his mildly impaired Left Ventricular Systolic Function (LVSD), a decision was made to introduce a His-bundle lead for synchronized pacing and protection against pacing-induced left ventricular dysfunction. He had a straight forward HIS pacing procedure with Medtronic Select Secure lead 3830. It is important to mention that during His bundle pacing procedure, we only got Selective His Bundle Pacing (S-HBP) at the high and low output with no evidence of local myocardial capture or Non-Selective His Pacing (NS-HBP). He has also got a small R wave sensing of 1 mV. Because of the fact that the patient is going to be pacing dependent following his AVN ablation, a decision made to implant a backup RV lead at apical RV septal position with Medtronic Solara MRI CRT-P generator. The HIS lead inserted in the left ventricle port and a right ventricular septal lead as a pack up in case of failed LV pacing. The usual programming was Bi-Ventricular (BiV) pacing with LV first and 80 msec VV delay so the RV pacing spikes falls in the refractory period of the ventricle and acts a safety mechanism in case of failed His capture. ECG and CXR following HBP (Figure 1).
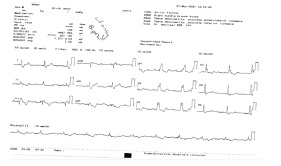
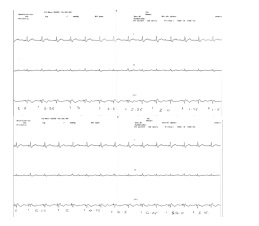
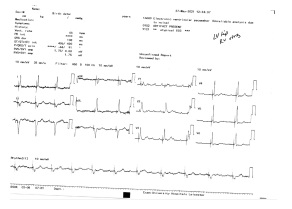
Four weeks later, the patient underwent the AVN ablation procedure which was uneventful. We have noticed a widening of the QRS complex and new Right Bundle Branch Block (RBBB) in his following ECG (Figure 3). The QRS duration has changed from 98 msec baseline to 148 msec with typical RBBB morphology and an isoelectric line following the pacing spike. Repeated pacing checks showed stable leads parameters with His threshold of 1V @ 0.4 msec. There was again no difference with a high and low output. Pacing at a maximum output of 8V @ 1sec failed to recruit any of the local myocardium with S-HBP through the process (Figure 4).
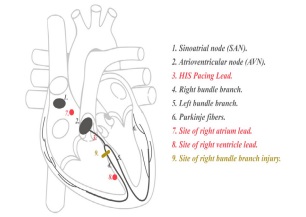
We decided to reprogram the device to BiV pacing with different VV delay settings trying to correct the blocked right bundle. This has led to a partial correction of RBBB. Interventricular delay of 30-50 msec with HIS pacing first to mimic the natural HV delay has shown the best outcome with QRS of 110 msec. However, lead V1 still shows some prominent and slight broad R waves due to apical to basal activation current of the interventricular septum (Figure 5).The anatomy of the conduction system, site of pacing, the proposed site injury to RBB and correction are illustrated in Figure 6.
We tested the HIS pacing in different unipolar settings and with Unipolar LV (HIS) tip to RV ring, we could achieve non selective HIS pacing with correction of the RBBB, QRS duration 108 msec (Figure 7). Due to high threshold for correction of RBBB at unipolar setting 2.5 V@ 0.5 msec, we opted for the first correction option of VV delay of 20 msec. However, the later remains a possible alternative option.
At 6 months’ follow up, the patient noted significant improvement of his exercise capacity and pacing checks remained stable.
Discussion
Owing to the dyssynchronous ventricular activation induced by Right Ventricular Pacing (RVP), HBP was found to be an effective alternative pathway to conventional RVP. For instance, several studies outlined the long term complications of VP and found an increased risk of wide QRS duration, left ventricular dysfunction, and prolonged hospitalization thus, there are several controversies regarding alternative pacing sites [3-5].
The PAVE study showed that for patients undergoing AV node ablation for AF, biventricular pacing provides a significant improvement in the 6-minute walk test and ejection fraction compared to rightventricular pacing. The benefits appear to be more pronounced in patients with heart failure [6].
Vijayramon and his group presented a data showing a significant improvement in LV function following AVN and HBP in patients with AF and difficult to control heart rate. The procedure was successful in 95% of patients. Left ventricular ejection fraction improved significantly during follow-up [7].
The variation of HIS bundle anatomy leads to different combination of S-HBP, NS-HBP and local myocardial capture [8]. In case of NS-HBP, the development of new RBBB will not cause any problem and might not be even noted as local myocardial capture is going to mask the development of RBBB. However, in cases were S-HBP only can be obtained; a new RBBB will lead to loss of the synchronized ventricular activation and the development of wide QRS. New RBBB can develop as a consquence of HBP or spontaneously.
The effect of HBP on RBBB located distal to site of pacing was discussed in a previous study done by Mahmud et al. They showed that during NS-HBP, higher pacing voltage completely corrected RBBB in 22/35 patients as compared to 5/18 patients at lower voltage. Remaining patients showed incomplete correction of RBBB. Lack of correction with S-HBP suggests that RBBB was distal to site of HBP. Voltage dependent correction of RBBB in NS-HBP suggests that conduction via a specialized parallel pathway maintains normal ventricular activation time [9].
To the best of our knowledge, correction of RBBB in patients with S-HBP, has not been described before. In our case, we described in details two possible methods of correction of RBBB either by combined HIS and RV septal pacing or by changing the pacing configuration to unipolar setting and testing different vectors.
Conclusion
New RBBB following S-HBP pacing can be achieved by 2 different mechanisms: Combined HIS/septal RV pacing and pacing HIS at different unipolar settings.
References
- Deshmukh P, Casavant DA, Romanyshyn M, Anderson K. Permanent, direct His-bundle pacing: A novel approach to cardiac pacing in patients with normal His-Purkinje activation. Circulation. 2000; 101: 869-877.
- Weijian Huang, Lan Su, Shengjie Wu, et al. Benefits of Permanent His Bundle Pacing Combined With Atrioventricular Node Ablation in Atrial Fibrillation Patients With Heart Failure With Both Preserved and Reduced Left Ventricular Ejection Fraction. J Am Heart Assoc. 2017; 6: e005309.
- Hussain MA, Furuya Kanamori L, Kaye G, Clark J, Doi SA. The Effect of Right Ventricular Apical and Nonapical Pacing on the Short- and Long-Term Changes in Left Ventricular Ejection Fraction: A Systematic Review and Meta-Analysis of RandomizedControlled Trials. Pacing and clinical electrophysiology: PACE. 2015; 38: 1121-1136.
- O’Keefe JH, Abuissa H, Jones PG, et al. Effect of chronic right ventricular apical pacing on left ventricular function. The American journal of cardiology. 2005; 95: 771-773.
- Sweeney MO, Hellkamp AS, Ellenbogen KA, et al. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation. 2003; 107: 2932-2937.
- R Dolshi, E Daoud, C Fellows, et al. Left Ventricular-Based Cardiac Stimulation Post AV Nodal Ablation Evaluation (The PAVE Study)(J Cardiovasc Electrophysiol. 2005; 16: 1160-1165.
- P Vijayaraman, F Subzposh, A Naperkowski. Atrioventricular node ablation and His bundle pacing. EP Europace. 2017; 19: iv10–iv16.
- V Nagarajan, S Yen Ho, S Ernst. Anatomical Considerations for His Bundle Pacing. Circulation: Arrhythmia and Electrophysiology. 2019; 1
- Rehan Mahmud, Shakeel Jamal. Effect of his bundle pacing on right bundle branch block located distal to site of pacing. Journal of Electrocardiology. 2020; S0022-0736(20)30602-6