
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Intracranial pressure monitoring: An unexpected diagnosis of obstructive sleep apnoea
Sogha Khawari*; Ahmed Toma
National Hospital for Neurology and Neurosurgery, London, United Kingdom.
*Corresponding Author: Sogha Khawari
National Hospital for Neurology and Neurosurgery,
United Kingdom.
Email: sogha.khawari@nhs.net
Received : Dec 24, 2021
Accepted : Jan 18, 2022
Published : Jan 25, 2022
Archived : www.jcimcr.org
Copyright : © Khawari S (2022).
Abstract
We present the case of a 45-year-old man who underwent intracranial pressure monitoring for postural headaches. ICP results were unexpected with crescendo of overnight pressures and sudden drops. A diagnosis of sleep-disordered breathing, in the form of obstructive sleep apnoea was suspected. Sleep-disorderd breathing is known to cause rise in ICP [1-3]. We discuss the importance of identifying OSA as a potential cause of headaches, and ICP wave forms that may suggest a potential diagnosis of obstructive sleep apnoea.
Keywords: intracranial pressure; intracranial pressure monitoring; obstructive sleep apnoea; sleep-disordered breathing.
Citation: Khawari S, Toma A. Intracranial pressure monitoring: An unexpected diagnosis of obstructive sleep apnoea. J Clin Images Med Case Rep. 2022; 3(1): 1610.
Background
Intracranial pressure (ICP) monitoring is a commonly used investigation in the neurosurgical field. The procedure is deemed low risk and over the years is carried out in growing number of cases, often for suspected cerebrospinal fluid (CSF) dynamic dysfunction. Normal ICP values also remains difficult to ascertain due to inability to perform ICP monitoring in healthy individuals due to ethical concerns. A systematic review by Norager et al [1] suggested ICP values in near-healthy individuals (e.g. telemetric ICP data in patient post small tumour resection as -5.9 to 8.3, however the overall sample size remains small and so the scarcity of normal pressures highlights the need for further research.
The different waveforms found in ICP monitoring have been described as A, B and C waves by Lundberg [2]. A-waves are seen in severe cases often suggesting poor outcome, B-waves are less understood with unclear clinical value and C-waves are physiological interactions between cardiac and respiratory cycles. It is currently agreed that B-waves are ICP oscillations of up to 50 mmHg occurring 0.5-2 times/minute, however the underlying physiology is not yet fully understood. Riedel et al [2] reported that nocturnal B-waves were found in association with sleep-disordered breathing. The study looked at ICP and polysomnographic data from 4 patients with no presumed gross structural abnormality; patients undergoing surgery for an incidental unruptured aneurysm. ICP data was taken 8 weeks post-surgery to allow for recovery, and was found to be within the normal range, however B-waves were seen during sleepdisordered breathing, i.e. apnoeic and hypopneic episodes. Although patients did not have known sleep-disordered breathing, all 4 patients showed a mild to severe range of sleepdisordered breathing. The study also found higher amplitude B-waves was seen in rapid eye movement (REM) sleep, and smaller waves in non-REM sleep stage.
Obstructive sleep apnoea (OSA) is the most common type of sleep-disordered breathing. Commonly caused by upperairway obstruction during sleep, leading to relative hypoxia and hypercapnia. Both these factors are thought to induce cerebrovascular vasodilation causing a rise in ICP. Jennum and Børgesen [3] showed that ICP increases during sleep, especially during non-REM sleep, and the duration of apnoea is strongly correlated to the elevation of ICP. Different stages of ICP changes has been described during apnoea; consisting of initial decrease, followed by a slow increase, and finally a steep increase in ICP, however these are not yet fully understood from a physiological perspective [3].
Case description
A 45-year-old man was referred by the headache specialist team for intracranial pressure monitoring for complex headaches. Headaches were persistent daily for several months, occipital in location, and associated with muffled hearing. Patient was known to have co-existing headaches which were more migrainous in nature. The history revealed worsening of symptoms early morning on waking, but also when stood upright after a prolonged time. Due to a history of lumbar surgery, initial investigations looked at ruling out a low-pressure state with potential CSF leak.
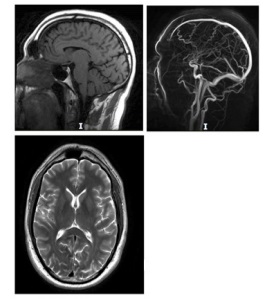
As part of investigations for the postural headache; the patient underwent MRI Head and Spine which showed no structural abnormality. Contrast sequences were obtained and ruled out signs of low intracranial pressure state. MR Venogram showed patent dural venous sinuses (Figure 1). As headache symptoms were worsening over coming months and impacted quality of life, the next investigation of choice was intracranial pressure monitoring over 24 hours. Patient was admitted and taken to the operating room for an intracranial pressure bolt insertion. A strain-gauge sensor was inserted into the right frontal cortex and tightened with a bolt.
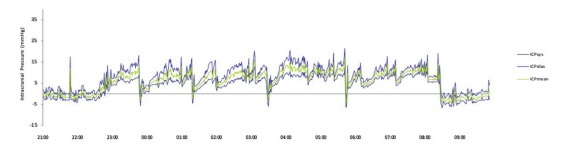
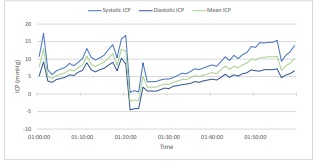
ICP data was collected and discussed in the hydrocephalus multidisciplinary meeting. ICP monitoring during the day was broadly in normal range, with a median systolic ICP of 5.082 mmHg, median diastolic ICP 0.947 mmHg and median ICP of 2.834 (Table 1). These were considered to be within the normal range. Overnight pressures were noted to be higher, with a median systolic ICP of 11.120 mmHg, median diastolic ICP 6.327mmHg and median ICP of 8.521 mmHg. Upon further reviewing the trend, ICP measurements displayed crescendo rises in pressures up to 21 mmHg, followed by intermittent drops in pressures to -5 mmHg (Figure 2 and 3), leading to a suspicion of sleep-disordered breathing.
Table 1:Displaying median ICP and pulse amplitude (mmHg) at daytime, night-time and 24-hour period.
Time period |
Median Systolic ICP |
Median Diastolic ICP |
Median ICP |
Median Pulse Amplitude |
All |
5.635 |
1.578 |
3.331 |
3.516 |
Day |
5.082 |
0.947 |
2.834 |
3.344 |
Night |
11.120 |
6.327 |
8.521 |
4.693 |
Following further collateral from the patient’s partner, history of snoring and witnessed apneas was elicited. This further built on the likely diagnosis of obstructive sleep apnoea, as part of sleep-disordered breathing. Patient was referred to the sleep team and a formal diagnosis was made. Patient started treatment with overnight continuous positive airway pressure (CPAP). On further outpatient follow up, the headaches had significantly improved.
Discussion
Our case report describes a potential sleep-disordered breathing diagnosis through ICP waveforms, a clinically important differential diagnosis when considering patients for ICP monitoring. Additionally, it offers an important addition to the very scarce literature on ICP monitoring in patients without structural brain abnormality, highlighting the normal ICP values are lower than previously thought. The report provides clear ICP monitor tracing with crescendo spikes and drops following interrupted sleep. The rises in pressure are thought to be related to obstructive sleep apnoea, whilst the drops in pressure are likely interrupted sleep with patient waking and sitting up. The relationship between OSA and rising ICP has been previously described [3-5]. Studies have shown a slow increase followed by a steep increase in ICP during sleep. Proposed causes are hypercapnia and hypoxia producing increase in intraarterial pressure and central venous pressure [3,4]. Further ICP data would provide better picture of the trend, particularly if coupled with sleep monitoring.
The case report highlights the complexity of understanding headaches. It emphasises on the importance of detailed history taking in patients presenting with headaches, in particular keeping in mind OSA symptoms. Earlier consideration of OSA can potentially avoid the invasive procedure of ICP monitoring. If ICP monitoring has been obtained, this case report outlines possible waveform to recognize as possible OSA.
References
- Norager NH, Olsen MH, Pedersen SH. et al. Reference values for intracranial pressure and lumbar cerebrospinal fluid pressure: a systematic review. Fluids Barriers CNS 18, 19. 2021. https://doi. org/10.1186/s12987-021-00253-4
- Riedel CS, Martinez-Tejada I, Norager NH, Kempfner L, Jennum P, Juhler M. B-waves are present in patients without intracranial pressure disturbances. J Sleep Res. 2021; 30(4): e13214. doi: 10.1111/jsr.13214.
- Jennum P, Børgesen SE. Intracranial pressure and obstructive sleep apnea. Chest. 1989; 95(2): 279-83. doi: 10.1378/chest.95.2.279.
- Wardly DE. Intracranial hypertension associated with obstructive sleep apnea: a discussion of potential etiologic factors. Med Hypotheses. 2014; 83(6): 792-7. doi: 10.1016/j.mehy.2014.10.011.
- Sugita Y, Iijima S, Teshima Y, Shimizu T, Nishimura N, Tsutsumi T, Hayashi H, Kaneda H, Hishikawa Y. Marked episodic elevation of cerebrospinal fluid pressure during nocturnal sleep in patients with sleep apnea hypersomnia syndrome. Electroencephalogr Clin Neurophysiol. 1985; 60(3): 214-9. doi: 10.1016/0013- 4694(85)90033-1.