
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Case report: Unusual infant methadone poisoning
Marjan Rashidan1; Pouneh Zolfaghari2; Mojtaba Ghasemian Aghmashadi3; Elahe Yahyaei4; Mohammad Bagher Sohrabi5*
1 Department of Microbiology, School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran.
2 Vice-chancellery of Health, Shahroud University of Medical Sciences, Shahroud, Iran.
3 Imam Hossain Center for Education, Research and Treatment, Shahroud University of Medical Sciences, Shahroud, Iran.
4 Vice-chancellery of Education, Shahroud University of Medical Sciences, Gorgan, Iran.
5 School of Medicine, Shahroud University of Medical Sciences, Shahroud, Iran.
*Corresponding Author: Mohammad Bagher
Sohrabi
School of Medicine, Shahroud University of Medical
Sciences, Shahroud, Iran.
Email: mb.sohrabi@yahoo.com
Received : Dec 12, 2021
Accepted : Jan 19, 2022
Published : Jan 26, 2022
Archived : www.jcimcr.org
Copyright : © Bagher Sohrabi M (2022).
Abstract
Poisoning with opioid compounds is one of the dangerous and unfortunately common poisonings of children in our country. The patient in question is a 5-month-old infant who inadvertently suffered from methadone syrup poisoning and was referred to the hospital with severe drowsiness and decreased level of consciousness. Fortunately, she was discharged in good general condition after initial diagnostic and appropriate treatment.
Keywords: methadone; poisonings; infant.
Citation: Rashidan M, Zolfaghari P, Aghmashadi MG, Yahyaei E, Sohrabi MB, et al. Case Report: Unusual infant methadone poisoning. J Clin Images Med Case Rep. 2022; 3(1): 1613.
Introduction
The patient was a five-month-old infant living in a village in Shahroud city (Northeastern Iran) who was referred to the emergency department of Imam Hossein Hospital in Shahroud by his mother at 6 pm. The patient’s mother explained that from about 1 pm the child had a decrease in the level of consciousness and severe drowsiness and did not respond well to external stimuli. The mother also mentioned that on the morning of the visit, the baby was completely healthy and had eaten well (breast milk). But the mother was forced to leave home due to the necessary work and left the infant to her seven-yearold sister. The infant has no history of any particular disease. She was the second child in the family and the result of cesarean delivery. Gestational age was 39 weeks and weighed 3350 grams at birth. She was hospitalized for three days at birth due to jaundice. The baby had been breastfed since birth and had received all the essential age-related vaccines. The education of the mother and father was a diploma.
In the examinations performed: BP: 90/55 mmHg, PR: 88 / min, RR: 9 /min, T: 37.4o C axillary, and GCS: 9-10. Child weight: 8 kg and on the 90th percentile, height: 63 cm between the 25th and 50th percentile, and head circumference: 43 cm on the 90th percentile.
The patient was severely drowsy and responded slowly to painful stimuli. The pupils were hypotonic and reacted to dim and symmetrical light. On examination of the head and neck, she was normocephaly and the anterior fontanelle was open and the posterior was closed. A small bruise and redness (2 X 3 cm) without hematoma was seen in the left temporalis area. The cervical spine had no particular problem. The chest was normal on examination. The abdomen was soft and had no organomegaly. The limbs were also in normal condition.
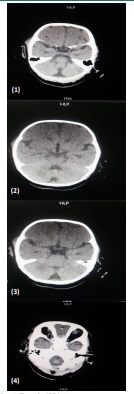
According to the patient’s condition, a suitable IV line was taken immediately for the patient. Necessary blood tests were taken including Arterial Blood Gases (ABG), Blood Cell Count (CBC), electrolytes (Na, k, Ca, P), blood sugar and etc. The test results are shown in Table 1. For the patient, saline sugar serum was started. Due to the redness of the temporal region due to the possibility of head trauma (the possibility of falling from the patient’s sister), a brain CT scan was performed, which fortunately did not have a specific point. The results of brain CT scan graphs are shown in Figures 1 to 4. Then the patient was prescribed 100 cc of hypertonic glucose 20%, but no particular reaction was seen. Due to the state of consciousness and pupils and the history of methadone syrup consumption by the infant’s father, by diagnosing methadone poisoning, Naloxone ampoules were also prescribed according to the protocol. Fortunately, after a few minutes, the baby’s consciousness improved and she began to cry. A closer interview with the parents revealed that the child’s father was in a state of drug withdrawal and was taking methadone syrup. The baby’s sister causes him to fall to the ground while playing with the infant. To soothe the baby’s crying, use the refrigerator’s syrup (methadone syrup) in the amount of one tablespoon (about 7 cc). Once the cause of drowsiness has been identified and a positive response to naloxone is given, the child was monitored in the intensive care unit and then in the pediatric ward, she was released from the hospital after 24 hours in good general condition and with full breastfeeding.
Table 1: Tests performed at referrals to Imam Hossain Hospital of Shahroud.
Testing |
Primitive |
CBC: |
10.7 |
ABG |
Normal |
ESR (1 hour) |
33 |
CRP (mg/dl) |
6.8 |
BUN (mg/dl) |
12 |
Cr (mg/dl) |
0.7 |
Blood sugar (mg/dl) |
73 |
Na (meqi/dl) |
138 |
K (meqi/dl) |
3.9 |
Ca (mg/dl) |
9.6 |
Phosphor (mg/dl) |
5.3 |
Alk-P (IU) |
403 |
ALT (IU) |
33 |
AST (IU) |
29 |
Total Bilirubin (mg/dl) |
2.6 |
Direct Bilirubin (mg/dl) |
0.7 |
Wright |
Negative |
Widal |
Negative |
Urine Analysis |
Normal |
Electro cardio ghraphy (ECG) |
Normal |
Chest x ray |
Normal |
CBC: Complete Blood Count; ABG: Arterial Blood Gases; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; BUN: Blood Urea Nitrogen.
Discussion
Substance abuse and its poisoning are known as the most common type of poisoning in the world. Due to the increase in population and the increase in the number of drug users, the resulting poisonings are spreading [1]. Also, it has been reported that the mortality rate in people who use drugs regularly is 13 times higher than in normal people [2]. According to the International Narcotics Control Board (INCB), 7.2% of the total population of Iran in 2018 used drugs. The drugs used included 34% opium, 27% crack, 19% heroin, 4% opium juice, 4% methamphetamine, and 2% cannabis [3]. Due to the increasing use of methadone at home to quit drugs, poisoning with it may occur accidentally in children or even adults with the aim of suicide or premeditated murder [1,2]. A review of the literature indicates the existence of numerous reports of intentional or accidental poisoning of children with methadone and its complications and death in Iran [3].
Methadone is a sedative and hypnotic drug derived from heroin [1]. It can be swallowed orally
The most common unintentional use in children is poisoning with drugs such as acetaminophen, heroin, and methadone. Methadone is a compound of the opioid-like d-phenyl proplamine that acts on the central nervous system by causing anxiety on the μ opioid receptor. Opioids usually act on receptors δ, μ, and κ in the brain to stimulate pain and analgesics [2-3]. Unlike other drugs, methadone is primarily taken orally, is easily absorbed in the intestines and stomach, has a longer shelf life (15-60 hours), is less tolerable, and is excreted late. Like other drugs, the main effects of methadone include relief, drowsiness, happiness, restlessness, and changes in perception and sensory perception [4]. Because of the properties of methadone, it is not surprising that methadone is commonly used to reduce pain, treat opioid dependence, store heroin and addictive drugs, and for pleasure and entertainment [5]. Although methadone is used by adults as an analgesic, analgesic, maintenance, pleasure, and entertainment, and to ward off poisoning, methadone is toxic and deadly to children. With the increase in methadone use in addictive drugs and drug and painkiller dependence, the number of children with methadone poisoning is constantly increasing [6,7]. Inadequate and unsafe storage method of methadone and non-standard conditions of its storage at home, especially in the presence of children at home for patients with methadone and drug users, although they do not want to poison children, primarily cause an increase in poisoning. Methadone poisoning of infants through breast milk, fetal period, and unwanted drug contamination have been reported [8]. In our country, methadone syrup does not have a specific glass, and addicts pour it into water bottles or other medicines and keep it at home. Unclear and unsafe methadone bottles or containers can cause this drug to be mistakenly used by parents or unknowingly by children themselves [1]. Storing methadone in a special container and glass would result in less methadone intake, less delay in the emergency room, and ultimately better poisoning for the child [3].
When opioids stimulate μ, δ, and κ receptors, they have effects such as happiness, restlessness, anxiety, depression, decreased respiration with increased carbon dioxide, pupil stenosis, relief, and analgesia [9]. Drugs are also known as anti-cough and constipation, suppressing the gastrointestinal tract [10]. The opium drug can also cause some acute neurovascular complications, often secondary to ischemia [11,12].
Unfortunately, due to the overuse of methadone in the form of withdrawal, today we are witnessing a significant increase in the incidence of poisoning with this drug [13]. More control needs to be exercised, especially through parents [14]. Finally, by educating addicts and their families about how to store methadone and making changes in the color, taste, and packaging of methadone syrup, as well as replacing methadone syrup with its tablets, it can be effective in reducing methadone poisoning in children [13-15].
In the patient in question, with the timely referral of the child, appropriate and rapid diagnosis and treatment, fortunately, the treatment was effective and the child was discharged in good general condition.
Declarations
Informed consent: Informed consent was obtained from all individual participants included in the study.
Consent for publication: Consent for publication: All named authors have seen and agreed on the submitted version of the paper. All persons in the acknowledgments section have agreed to that inclusion.
Availability of data and material: The dataset used and/or analyzed during the present study is available from the corresponding author upon reasonable request.
Conflict of interests: The authors declared that they have no conflict of interest.
Funding: This study received funding from the research deputy of Shahroud University of Medical Sciences.
Authors’ contributions: All authors of this article have played an active role in all aspects of the preparation of the article and final approval of the version to be published.
Acknowledgment: We hereby acknowledge the research deputy. Also, we would like to thank all participating patients.
References
- Mehrpour O, Hoyte C, Amirabadizadeh A, Brent J. Clinical characteristics and time trends of hospitalized methadone exposures in the United States based on the Toxicology Investigators Consortium (ToxIC) case registry: 2010–2017. BMC Pharmacol Toxicol. 2020; 21: 53.
- Alinejad S, Kazemi T, Zamani N, Hoffman RS, Mehrpour O, et al. A systematic review of the cardiotoxicity of methadone. EXCLI J. 2015; 14: 577–600.
- Jabbehdari S, Farnaghi F, Shariatmadari SF, Jafari N, Mehregan FF, et al. Accidental Children Poisoning With Methadone: An Iranian Pediatric Sectional Study. Iran J Child Neurol. 2013; 7: 32–34.
- Giorgetti A, Pascali J, Montisci M, Amico I, Bonvicini B, Fais P, et al. The Role of Risk or Contributory Death Factors in Methadone-Related Fatalities: A Review and Pooled Analysis. Metabolites. 2021; 11: 189.
- George M, Kitzmiller JP, Ewald MB, Katherine A, Becter ML, Salhanick S. Methadone Toxicity and Possible Induction and Enhanced Elimination in a Premature Neonate. J Med Toxicol. 2012; 8: 432–435.
- Gaither JR, Leventhal JM, Ryan SA, Camenga DR. National Trends in Hospitalizations for Opioid Poisonings Among Children and Adolescents, 1997 to 2012. JAMA Pediatr. 2016; 170: 1195–1201.
- Chen X, Wang Y, Yu X, Schoenfeld E, Saltz M, Saltz J, et al. Largescale Analysis of Opioid Poisoning Related Hospital Visits in New York State. AMIA Annu Symp Proc. 2017; 2017: 545–554.
- Boyer EW, McCance-Katz EF, Marcus S. Methadone and buprenorphine toxicity in children. Am J Addict. 2011; 19: 89-95.
- Mistry V, Jeffery AJ, Madira W, Padfield CJ, Rutty GN, et al. Methadone toxicity in infants: A report of two fatalities. Forensic Sci Med Pathol. 2010; 6: 116-120.
- Kintz P, Evans J, Villain M, Cirimele V. Interpretation of hair findings in children after methadone poisoning. Forensic Sci Int. 2010; 196: 51-54.
- Sidlo J, Valuch J, Ocko P, Bauerová J. Fatal methadone intoxication in a 11-month-old male infant. Soud Lek 2011; 54: 23-25.
- Hon KL, Leung TF, Hung CW, Cheung KL, Leung AK, et al. Ingestion--associated adverse events necessitating pediatric ICU admissions. Indian J Pediatr. 2009; 76: 283-286.
- Glatstein M, Finkelstein Y, Scolnik D. Accidental methadone ingestion in an infant: Case report and review of the literature. Pediatr Emerg Care. 2009; 25: 109-111.
- Lebin JA, Chen BC, Valento MJ. Reversal of Pediatric Opioid Toxicity with Take-Home Naloxone: A Case Report. J Med Toxicol. 2019; 15: 134–135.
- Lumba P, Medows M, Lumba H, Bray L. Methadone Toxicity in a Pediatric Patient: A Case Report. Cureus. 2021; 13: e14860.