
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Radio clinico histological presentation of intracranial dural chondroma
Yehouenou Tessi Romeo Thierry1*; Dokponou Yao Christian Hugues2 ; El Kacemi Inas3 ; Gazzaz Miloud4
1Department of Radiology, Mohammed V Military Teaching Hospital, Mohammed V University, Rabat, Morocco. 2 Department of Neurosurgery, Mohammed V Military Teaching Hospital, Mohammed V University, Rabat, Morocco. 3 Consultant, Department of Neurosurgery, Mohammed V Military Teaching Hospital, Mohammed V University, Rabat, Morocco. 4 Professor of Neurosurgery, Director of Neurosurgery training program, Mohammed V Military Teaching Hospital, Mohammed V University, Rabat, Morocco.
*Corresponding Author: Yehouenou Tessi Romeo
Thierry
Department of Radiology, Mohammed V Military
Teaching Hospital, Mohammed V University, Rabat,
Morocco
Email: nactessi@yahoo.fr
Received : Dec 06, 2021
Accepted : Jan 19, 2022
Published : Jan 26, 2022
Archived : www.jcimcr.org
Copyright : © Yehouenou Tessi RT (2022)
Keywords: chondroma; intracranial; dural; clinical; CT scan; MRI; anatomopathology
Citation: Yehouenou Tessi RT, Dokponou YCH, El Kacemi I, Miloudi G. Radio clinico histological presentation of intracranial dural chondroma. J Clin Images Med Case Rep. 2022; 3(1): 1615.
Description
We report a challenging diagnosis and the successful management of a rare case of intracranial dural chondroma in a 19-year-old student. He was admitted for secondary epilepsy with behavioral and mood disorder without neurological deficit. His past medical history was unremarkable. The patient was initially taken, by his parents, to the psychiatry department, where medical treatment was prescribed. The cerebral MRI was done, and based on the extra-axial, left fronto-parietal lesion found. Plus, the nonspecific aspect of the clinical findings, the radiological investigations did not help for a straight forward diagnosis orientation. The patient underwent surgery and promptly recovered after the gross total resection of the tumor.
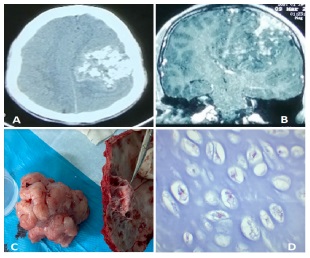
Intracranial chondroma of dural origin is a rare (incidence less than 0,5% of all intracranial tumors) and even exceptional type of chondromas. The first case reported by Hirschfeld in 1851. Chondromas are benign tumors composed of mature hyaline cartilage. The clinical symptoms are variable and due to mass effect depending on the size and location of the lesion (Headache 52.5%, Diplopia 11.9%). It has been reported more frequently at the skull base, less regularly at the falxcerebri, and exceptionally of the dura, when it happened to be intracranial [1,2]. CT scan shows a cerebral tumor with calcifcation and bone erosion due to the tumoral infiltration. Moreover on MRI, the tumor parenchyma appeared heterogeneously hyposignal on T1WI and hypersignal or mixed hypersignal and hyposignal on T2WI, inhomogeneous enhancement on postcontrast (Figure 1). The differential diagnosis with other dural origin tumors like meningioma may not be certain before surgery. The diagnosis confirmation requires a histopathological finding (Figure 1D).
References
- Sullivan JC, Goldsmith J, Rojas R, Varma H, Kasper EM. Intracranial dural parafalcine chondroma: Case report and systematic review of the literature. World neurosurgery. 2019; 122: 1-7.
- Reinshagen C, Redjal N, Sajed DP, Nahed BV, Walcott BP, et al. Intracranial dural based chondroma. Journal of Clinical Neuroscience. 2016; 25: 161-163.