
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Laparoscopic management of cholecystoduodenal fistula: A case report
Himanshu Prasad1*; Geeta Ghag2 ; Vipul Nandu3
1Resident, Department of General Surgery, Hinduhridaysamrat Balasaheb Thackeray Medical College and Dr. Rustom Narsi Cooper Municipal General Hospital, Mumbai, India. 2 Professor, Department of General Surgery, Hinduhridaysamrat Balasaheb Thackeray Medical College and Dr. Rustom Narsi Cooper Municipal General Hospital, Mumbai, India. 3 Assistant Professor, Department of General Surgery, Hinduhridaysamrat Balasaheb Thackeray Medical College and Dr. Rustom Narsi Cooper Municipal General Hospital, Mumbai, India.
*Corresponding Author: Himanshu Prasad
Resident, Department of General Surgery, Hinduhridaysamrat Balasaheb Thackeray Medical College and
Dr. Rustom Narsi Cooper Municipal General Hospital,
Mumbai, India.
Tel: +91-9414594118
Email: himanshuprasad1@gmail.com
Received : Dec 27, 2021
Accepted : Jan 20, 2022
Published : Jan 27, 2022
Archived : www.jcimcr.org
Copyright : © Prasad H (2022)
Abstract
Fistula between gall bladder and gastrointestinal tract occurs anywhere for example stomach, duodenum, and colon. Results of inflammatory reaction adhesion may be occur and between two organs and gall stone’s pressure may be contribute this process. Laparoscopic cholecystectomy has been the most widely accepted modality of treatment for patients with gall bladder disease. With time and increasing experience laparoscopic cholecystectomy is now being successfully attempted to treat almost all benign gall bladder pathology and their complications. One such uncommon infrequent complication of cholecystolithiasis is the cholecystoenteric fistula. Management of cholecystoduodenal fistula was traditionally performed by open method. With increasing newer laparoscopic techniques and advancement in the field, cholecystoduodenal fistula, an uncommon clinical entity is now being successfully treated via laparoscopic approach. It is feasible and safer than the conventional open approach in experienced hands, thus decreasing the overall morbidity and mortality attributed to the condition. We report a case of 55yr old female with cholecystoduodenal fistula treated successfully by laparoscopic approach using an Endovascular Gastro-Intestinal Anastomosis (GIA endo) stapler at H.B.T. Medical College & Dr. R.N. Cooper Municipal General Hospital, Juhu, Mumbai.
Keywords: cholecystoduodenal fistula; laparoscopic cholecystectomy.
Citation: Prasad H, Ghag G, Nandu V. Laparoscopic management of cholecystoduodenal fistula: A case report. J Clin Images Med Case Rep. 2022; 3(1): 1616.
Case report
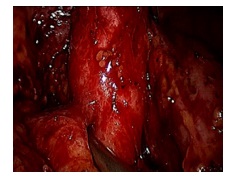
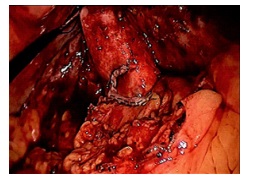
A 55-year-old female presented to OPD with complaints of right sided abdominal pain for past 1 month on and off associated with occasional vomiting and intolerance to fatty meals. Patient had history of acute abdominal illness 2 years ago for which she was diagnosed as cholelithiasis. She was asymptomatic following that and came to us with above mentioned complaints for a month. On clinical examination patient had mild pallor and icterus, abdomen was soft with focal tenderness over right hypochondrium and epigastric region. Laboratory investigations revealed raised serum bilirubin and liver enzymes. Ultrasound imaging showed pneumobilia suggestive of bilioenteric fistula, hence MRCP and contrast CT scan was done which clearly demonstrated bile flow from gall bladder to 1st part of duodenum with stone of size 1.5 X 1 cm in gall bladder and of size 9 mm obstructing at the terminal common duct. Diagnostic laparoscopy was done which revealed dense omental adhesions and fat stranding covering the gall bladder fossa and inferior surface of liver as shown in (Figure 1). Adhesiolysis was done duodenum was seen in close proximity to liver and adherent to it. A window was created between gall bladder, communication duodenum and the liver isolating the fistulous to gall bladder as in (Figure 2).
GIA Endo stapling device inserted inside and gently passed into the space and stapling of the duodenal wall from the fistula was done releasing the gall bladder from duodenum. Calot’s triangle dissected and routine laparoscopic cholecystectomy was performed. Patient tolerated orals on POD-1 and discharged. Immediate and late post-operative period was uneventful. Patient was followed up for a year with review imaging and no complications or residual disease noted.
Discussion
With time and increasing experience laparoscopic cholecystectomy is now being successfully attempted to treat almost all benign gall bladder pathology and their complications [1]. One such uncommon complication is the cholecystoenteric fistula, an abnormal spontaneous tract with bile drainage from gall bladder to adjacent bowel loops. Though it is uncommon it is a well-recognized complication of gall stone disease (75%) [2,3].
Gall stone ileus a dramatic clinical presentation of a cholecystoenteric fistula, is reported in 8% to 20% of patients. Although most fistula between gall bladder and intestinal tract becomes obvious pre-operatively or intra-operatively, certain fistula are insidious and may not be appreciated even at surgery [4,5]. We share our experience on a case of cholecystoduodenal fistula diagnosed pre-operatively and managed successfully by laparoscopic approach using endo GIA stapling technique.
Cholecystoenteric fistulas are more common in female geriatric population. Due to nonspecific symptoms the diagnosis of cholecystoenteric fistula is very difficult unless ultrasound shows pneumobilia or there is an indication for more advanced diagnostic modalities like CT, MRCP or ERCP [6].
At the inception of laparoscopic surgery and till recently cholecystoduodenal fistula is considered a contraindication for laparoscopic cholecystectomy and the standard treatment was open cholecystectomy with duodenal repair. With advancement in laparoscopic procedures many reports have described various laparoscopic approach to cholecystoduodenal fistula. In addition, cholecystoenteric fistula has been successfully managed using staplers in several cases with the advent of endoscopic stapling devices and increasing technical ability of laparoscopic surgeons. However bleeding, local adhesions and technical difficulty are usually encountered during laparoscopy and the rate of conversion to open surgery is very high (58.8%) [7,8-11].
Laparoscopic intestinal stapling devices are found to be much safer and flexible and is now the preferred and widely accepted treatment of choice for cholecystoduodenal fistula.
Conclusion
Cholecystoduodenal fistula is no longer a contraindication to laparoscopic surgery and in expert hands, it is safe and ideal. Although it requires meticulous handling and dissection to successfully perform the procedure, it decreases the overall morbidity and mortality providing all advantages of minimal invasive surgery. Endoscopic stapling technique is the widely accepted treatment of choice for cholecystoduodenal fistula.
Conflicts of interest: No conflicts of interests or disclosures.
References
- Cuschieri A, Dubois F, Mouiel J. The European experience with laparoscopic cholecystectomy. Am J Surg. 1991; 161: 385-7.
- Chowbey PK, Bandyopadhyay SK, Sharma A. Laparoscopic management of cholecystoenteric fistulas. J Laparoendosc Adv Surg Tech A. 2006; 16: 467-72.
- Angrisani L, Corcione F, Tartaglia A. Cholecystoenteric fistula (CF) is not a contraindication for laparoscopic surgery. Surg Endosc. 2001; 15: 1038-41.
- Sharm A, Sullivan M, English H, Folwy R. Laparoscopic repair of cholecystoduodenal fistula. Surglaparosc Endosc. 1994; 4: 433- 5.
- Ibrahim IM, Wolodiger F, Saber AA. Treatment of cholecystocolonic fistula by laparoscopy. Surg Endosc. 1995; 9: 728-9.
- Dash N. Successful laparoscopic management of four cases of cholecystoduodenal fistula. Med J. Armed Forces India. 2012; 68(1): 88.
- Moreno FR, Suescun RG, Martínez JF, Hidalgo JG, Espadas BP, Hernández JC. Treatment of cholecystoduodenal fistula in the era of laparoscopy. Spanish journal of digestive diseases: official organ of the Spanish Society of Digestive Pathology. 2001; 93(11): 715-20.
- Wang WK, Yeh CN, Jan YY. Successful laparoscopic management for cholecystoenteric fistula. World J gastroenterol. 2006; 12(5): 772-5.
- Latic A, Latic F, Delibegovic M, Samardzic J, Kraljik D, Delibegovic S. Successful laparoscopic treatment of cholecystoduodenal fistula. Med Arh. 2010; 64: 379-80.
- Abou-Saif A, Al-Kawas FH. Complications of gallstone disease: Mirizzi syndrome, cholecystocholedochal fistula, and gallstone ileus. Am J Gastroenterol. 2002; 97(2): 249.
- Csendes A, Diaz JC, Burdiles P, Maluenda F, Nava O. Mirizzi syndrome and cholecystobiliary fistula: a unifying classification. Br J Surg. 1989; 76(11): 1139-43.