
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Breakthrough infection in covid 19: Indian scenario
Sheetal Goenka1; Dimple Kasana2*
1Post Graduate Resident, Department of Microbiology, Vardhman Mahavir Medical College, Delhi, India.
2Director Central Research Institute, Kasauli, India.
*Corresponding Author: Dimple Kasana
Director Central Research Institute, Kasauli, India.
Email: dimplekasanacri@gmail.com
Received : Dec 29, 2021
Accepted : Jan 20, 2022
Published : Jan 27, 2022
Archived : www.jcimcr.org
Copyright : © Kasana D (2022).
Abstract
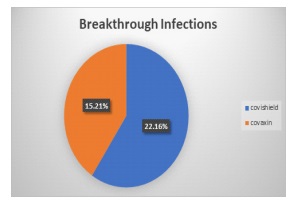
The Coronavirus disease 2019 (COVID19) mass vaccination program in India began on January 16, 2021, with two vaccines: Covishield and Covaxin. One of the most important things to remember is that, while COVID-19 immunizations offer the highest protection, but do not stop us from catching the virus. It protects us from acquiring serious illnesses, lowers the possibility of hospitalization, and minimizes the risk of mortality. In many countries, including India, breakthrough infections in fully vaccinated persons have been observed. When a fully vaccinated individual contracts the SARs-COV-2 virus, it is known as a breakthrough infection. With a large population vaccinated, many breakthrough cases have come to the forefront. It is believed that vaccinated individuals either remain asymptomatic or develop mild to moderate symptoms. In certain cases, depending on the person’s age, pre-existing comorbidities, he or she may succumb to the virus. However, the chances are very rare. When we compared the data of breakthrough infection in terms of percentage, Covishield 22.16 percent, Covaxin 15.21 percent people got, but the disease was mild or asymptomatic.
Citation: Goenka S, Kasana D. Breakthrough infection in covid 19: Indian scenario. J Clin Images Med Case Rep. 2022; 3(1): 1618.
Introduction
Despite our advancement in medical science and research, we are always be challenged with new pathogens that create a danger to human lives, the health care system, and economic security. New infectious pathogens are discovered every day. Throughout history, epidemics and pandemics have been accountable for thousands of lives lost. Just recently, almost every country in the world has been affected by the global virus pandemic. Coronavirus disease 2019 (COVID-19) is an infectious disease caused by a newly discovered coronavirus. On December 31, 2019, the coronavirus outbreak came to light when the health authority of China reported a cluster of cases of pneumonia of unknown etiology. These patients presented with breathing difficulty, dry cough, fever, body pain, generalized weakness in the capital of China’s Hubei province Wuhan, China. The disease eventually spread to other provinces in China, as well as the rest of the world. A large number of cases were related to the Huanan fresh food market, where a variety of seafood is available for sale [1]. This COVID-19 pandemic has reached every country in the world, with 9.93 million people infected. On January 30, 2020, India reported the first case of coronavirus in the southern state of India, Kerala [2]. Since then, Covid 19 virus infection has spread across all the states.
When a Coronavirus infected individual breathes, speaks, laughs, sings, coughs, or sneezes, droplets and virus particles are discharged into the air, spreading the coronavirus (Covid 19). Larger droplets may fall to the ground in a matter of seconds, but tiny infectious particles can persist in the air and concentrate in enclosed spaces, particularly where a large number of people are present and ventilation is poor. COVID-19 prevention necessitates the use of masks, hand cleanliness, and physical separation. Coronaviruses is Single-stranded RNA viruses with having envelope, membrane, and nucleocapsid are essential structural proteins [3]. They have a higher mutation rate and a propensity for recombination than DNA viruses, allowing them to adapt to new hosts and ecological niches. Alpha, beta, delta, and gamma are the four major subgroups of coronaviruses that are widely distributed in mammals and birds, but till now, only alpha and beta are known to cause disease in humans. Respiratory, enteric, cardiovascular, and neurological conditions are all caused by these viruses. Humans have been infected with seven coronaviruses that originated in bats, rodents, or domestic animals.
The common cold and other respiratory-related symptoms are caused by four coronaviruses: including 2 alpha coronaviruses (229E, NL63) and 2 beta coronaviruses (OC43, HKU1) [4]. Furthermore, three beta coronaviruses are known to cause respiratory syndromes with high mortality rates in humans: severe acute respiratory syndrome coronavirus-1 (SARS-CoV-1; an outbreak in 2002-2003 with 8096 cases and 774 deaths worldwide), Middle East respiratory syndrome coronavirus (MERSCoV; an outbreak in 2012 with 2494 cases and 858 deaths), and severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) responsible for the ongoing pandemic and Coronavirus disease (COVID-19) [4,5]. The viral load in the upper respiratory tract peaks around the time of symptom start, and viral shedding occurs 2 to 3 days before symptoms appear. Asymptomatic and presymptomatic carriers can transmit SARS-CoV-2 [6].
SARS-CoV-2 targets cells such as nasal and bronchial epithelial cells and pneumocytes early in infection via the viral structural spike (S) protein, which binds to the angiotensin-converting enzyme 2 (ACE2) receptor. The type 2 transmembrane serine protease (TMPRSS2), present in the host cell which promotes viral uptake by cleaving ACE2 and activating the SARS-CoV-2S protein, which mediates coronavirus entry into host cells. The angiotensin-converting enzyme 2 and the type 2 transmembrane serine protease are expressed in host target cells, particularly alveolar epithelial type cells [6].
The Second wave of coronavirus in India came as a double whammy. Since April, India has seen an increase in Covid-19 infections, with over 3 lakh new cases being reported per day. The two vaccines being (Covishield and Covaxin) administered in India right now claim to offer protection of 78 percent and 79 percent, respectively, against symptomatic Covid-19 disease. The fear of the third wave is still there with a spike in new cases in some parts of the country. The R-value of Kolkata, Bengaluru, and Mumbai is hovering near 1, which further triggers the fear of another round of surge in Coronavirus infections. Governments and experts have been advising people to follow Covid-19 protocols such as wearing marks, maintaining distance, and avoid crowding in order to limit spike in Covid-19 cases.
It has been over a year and a half since the novel coronavirus impacted our lives in the most unprecedented ways. Now, with the vaccines available, people have become more relaxed, less vigilant, but still at risk. The COVID19 mass vaccination program in India began on January 16, 2021, with two vaccines: Covishield and Covaxin. The vaccines approved and deployed in India by the regulatory authority included AZD1222 - ChAdOx1- S (Covishield), manufactured in India by Serum Institute of India through a license from AstraZeneca-Oxford and BBV152 (Covaxin)indigenous vaccine developed by Bharat Biotech in collaboration with the Indian Council of Medical Research (ICMR) [7]. It is SARS-CoV-2 Spike (S) glycoprotein is encoded by a recombinant, replication-deficient chimpanzee adenovirus vector. Folowing administration, the coronavirus’s part genetic material is expressed, triggering an immunological response, it is manufactured by Astra Zeneca and Covaxin by Bharath Biotech and Indian Council of Medical Research [7], which is a whole-Virion Inactivated Vero Cell-derived platform technology, because inactivated vaccines do not multiply, they are unlikely to revert and cause disease. It carries dead viruses that are unable to infect humans but can able to instruct the immune system to mount a defensive response against infection [8].
As of now, more than 290 million Indians have been completely vaccinated [9]. In many countries, including India, breakthrough infections in fully vaccinated persons have been observed [10].
COVID-19 has also shown us how quickly a disease can spread over the globe in a small span of time. Looking at how COVID-19 began in Wuhan in December of 2019; by the 19th of May of 2020, there had been 4, 894 098 coronavirus illnesses and 320, 180 deaths globally. According to the Worldometer, there were 134, 641, 215 coronavirus cases and 2, 917, 995 fatalities worldwide as of April 9th, 2021. This demonstrates how severe the COVID-19 is and how it has influenced the entire world in such a short period of time. To put an end to the catastrophe, a significant part of the population must be immune to the virus. Vaccination is the safest approach to accomplish this. Vaccines are a technique that humanity has relied on to reduce the mortality toll from infectious diseases in the past.
Aim: Our study aimed to determine the incidence of breakthrough infections in the covid-19 patient in north India.
Material and methods
During the specified period from September–October 2021 the data was collected by online survey using populate social media tool. The results included the responses of 500 individuals, all of them were are Indian inhabitants.
Results
Table 1:Data related to Covaxin.
Covaxin Vaccine |
Total no of cases |
Positive after vaccine |
1st dose |
28 |
19 |
2nd dose |
18 |
7 |
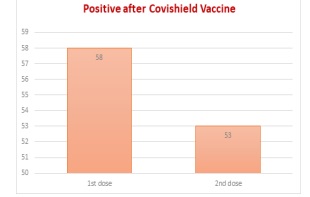
During the survey, a total of 500 responses were collected among which males were 307 and female were 193. A total of 284 people were vaccinated, 138 of them had received the partial dose of the Covid 19 vaccine, with 146 subsequently received the complete doses of the two-dose vaccine as recommended. The vaccine administered was either Covishield or Covaxin. While 238 individuals had received Covishield, 8 had got Covaxin complete doses. Our data analysis included breakthrough infections that occurred after 14 days of the 2nd dose administration in 60 people. When we compared the data of breakthrough infection in terms of percentage, Covishield 53 (22.16%), Covaxin 7 (15.21%), but the disease was mild or asymptomatic. The majority of breakthrough infections occurred in health care workers (46), rest 14 were non-healthcare workers.
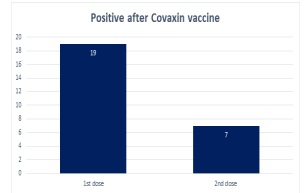
Table 2:Data related to Covishield.
Covishield Vaccine |
Total no. of cases |
Positive after vaccine |
1st dose |
110 |
58 |
2nd dose |
128 |
53 |
Discussion and conclusion
COVID-19 has taught individuals about the importance of public health measures, as well as the critical importance of lung health. COVID-19 has made it evident that every breath matters. So, whether quitting smoking or seeking to better manage lung diseases, people are more aware of their lung health. The worldwide effort to develop a COVID-19 vaccination that is both safe and effective is bearing fruit. Almost two dozen vaccines have already been approved around the world, with many more in the works.
The vaccine doesn’t provide 100 percent protection from the risk of infection of Coronavirus but instead aids in reducing the severity of infection. In our study, none of the breakthrough infection was severe or needed hospitalization, oxygen supplementation. All recovered in home isolation. The majority of breakthrough infections occurred in health care workers who received both doses of vaccine. They also did not face any severe symptoms needing ICU care or resulting in mortality. The number of cases after Covishield is more as compared to Covaxin because the number of doses given is more in Covishield in comparison to Covaxin.
Covishield and Covaxin both have a two-dose regimen. Their effectiveness takes at least 14 days to work after the second dose. Their efficacy kicks in at least two weeks after the second dose.
To keep the number low, it is critical to take appropriate public health measures like wearing a mask and social distancing. Because the vaccination does not ensure complete protection against Covid-19 infection, it instead reduces the disease’s severity and course of the disease generally stays mild to moderate and reduces mortality due to covid19 infection. There are a lot of factors that can increase risk of developing a breakthrough infection. The prime reason is the new emerging variants. They are said to be highly transmissible and may be able to evade vaccine-induced immunity. Given that COVID vaccines were developed with respect to the original COVID strain, new variants may dodge the antibodies provided by the vaccines.
Therefore, authors recommend the Covid 19 appropriate behavior to continue irrespective of vaccination status.
References
- Siddiqui AF, Wiederkehr M, Rozanova L, Flahault A. Situation of india in the COVID-19 pandemic: India’s initial pandemic experience. International Journal of Environmental Research and Public Health. 2020; 17(23): 1-18.
- Saxena S, Manchanda V, Sagar T, Nagi N, Siddiqui O, Yadav A, et al. Clinical characteristic and epidemiological features of SARS CoV-2 disease patients from a COVID-19 designated hospital in New Delhi. Journal of Medical Virology. 2021; 93(4): 2487-92.
- Almaghaslah D, Kandasamy G, Almanasef M, Vasudevan R, Chandramohan S. Review on the coronavirus disease (COVID-19) pandemic: Its outbreak and current status. International Journal of Clinical Practice. 2020; 74(11): 1-9.
- Bennet BM, Wolf J, Laureano R, Sellers RS. Review of Current Vaccine Development Strategies to Prevent Coronavirus Disease 2019 (COVID-19). Toxicologic Pathology. 2020; 48(7): 800-9.
- Schoeman D, Fielding BC. Coronavirus envelope protein : current knowledge. 2019; 01: 1-22.
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA - Journal of the American Medical Association. 2020; 324(8): 782-93.
- Delhi N. Title Breakthrough infection with SARS-CoV-2 and its predictors among healthcare workers in a medical college and hospital complex in Delhi, India. 2021; 1-11.
- Harapan H, Itoh N, Yufika A, Winardi W, Keam S, Te H, et al. Coronavirus disease 2019 (COVID-19): A literature review. Journal of Infection and Public Health [Internet]. 2020; 13(5):667-73.
- Tyagi K, Ghosh A, Nair D, Dutta K, Singh P. Since January 2020 Elsevier has created a COVID-19 resource centre with free information in English and Mandarin on the novel coronavirus COVID- 19. The COVID-19 resource centre is hosted on Elsevier Connect, the company’ s public news and information. 2020: 2020-2.
- J BP, Jolly B, John N, Bhoyar RC, Majeed N, Senthivel V, et al. Genomic survey of SARS-CoV-2 vaccine breakthrough infections in healthcare workers from Kerala, India. Journal of Infection. 2021; (xxxx): 7-10.