
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Rare oncological metastasis; Colorectal and male breast cancer
Walid Shalata1*; Mitchell Golosky2 ; Sofia Man1 ; Omar Abu-Saleh1 ; Yusuf Khalaila3 ; Mohamed Haj3 ; Alexander Yakobson1
1 The Legacy Heritage Oncology Center & Dr. Larry Norton Institute, Soroka Medical Center & Ben-Gurion University, Beer-Sheva, Israel. 2 Medical School for International Health and Sciences, Ben-Gurion University, Beer-Sheva, Israel. 3 Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel.
*Corresponding Author: Walid Shalata
Resident Physician of Oncology, The Legacy Heritage
Oncology Center & Dr. Larry Norton Institute, Soroka
Medical Center & Ben-Gurion University, Beer-Sheva,
Israel.
Cell: +972 (0)54 2967100;
Email: walid.shalata@gmail.com
Received : Dec 12, 2021
Accepted : Jan 21, 2022
Published : Jan 28, 2022
Archived : www.jcimcr.org
Copyright : © Shalata W (2022).
Abstract
In this report, we describe three cases of rare oncologic metastases. The first patient was a 73-year-old male, diagnosed with metastatic male breast cancer after radiological investigation of suspected renal cell carcinoma. The other two male patients, a 69 and 73-yearold, were diagnosed with colon adenocarcinoma; suspected to be a second primary prostate carcinoma following Positron Emission Tomography-Computer Tomography (PET-CT). This suspicion was ruled out by prostatectomy and histopathological investigations, which instead found adenocarcinoma of colonic origin.
Keywords: rare metastasis; colon cancer; male breast cancer; second primary; adenocarcinoma
Citation: Shalata W, Golosky M, Man S, Abu-Saleh O, Khalaila Y, et al. Rare oncological metastasis; Colorectal and male breast cancer. J Clin Images Med Case Rep. 2022; 3(1): 1620.
Introduction
Male breast cancer is a very rare malignancy among men, representing approximately 1% of all cancers in men, and less than 1% of all breast cancers overall [1]. Due to the rarity of the disease, there has been a scarcity of clinical trials carried out, leaving male breast cancer data and literature based primarily on a limited number of case reports. Presently, treatment options are generalized from the management of female breast cancer data [2,3]. In a well-documented study involving 778 cases of breast carcinoma involving the male breast, 98% of these cases were primary cancers. Of those considered to be metastases from an alternative site of origin, 58% were from cutaneous melanomas [2]. Primary male breast cancer was found to metastasize in 26% of patients studied, with 56% having disease recurrence in the bone, 51% in the lung, and 17% in the liver [4]. Metastases to the breast from other sources in male patients are seldom found and are instead presumed to be primary breast carcinomas [5]. Additionally, metastases involving the breast in men is 5-6 times less likely than in females [6]. A case study reported an 80-year old male patient with metastatic adenocarcinoma of the prostate that spread to the right breast and was initially confused with gynaecomastia [7]. It is noted that male breast cancer patients should be carefully monitored for the occurrence of a second primary cancer, with one study finding that 12% developed a second primary cancer [8]. The most common secondary primary cancers were found to be a second breast cancer (SIR = 52.12, 95% CI = 31.83-80.49), cutaneous melanoma (SIR = 2.98, 95% CI = 1.63–5.00) and stomach cancer (SIR = 2.11, 95% CI = 1.01–3.88) [8-10]. In the present case study, we present a unique case of a male patient presenting with suspected renal cell carcinoma, later confirmed to be metastatic breast cancer.
In the literature, cancers of the colon, rectum and anus are frequently combined as colorectal cancer for the purposes of uniformity. In terms of the global burden, the incidence of colorectal cancer is third behind lung and breast cancers respectively. When considering mortality, colorectal cancer increases to second, only behind lung cancer as the most common cause of cancer death around the world [11]. Men with colorectal cancer have been found to be at a significantly increased risk of developing a second primary prostate cancer (HR = 2.30, 95% CI = 2.18-2.43; P < 0.001), even more so than a second primary colorectal cancer. This has been demonstrated to be true for men under the age of 65 and age 55 [9,10]. Men with second primary prostate cancer subsequent to a first primary colorectal cancer, were shown to preferentially die from prostate cancer [9]. Approximately 50% of patients with colorectal cancer later develop metastasis of the primary cancer [12]. Collectively, these distant metastases are known to be a major threat to treatment success, thereby reducing the overall patient outcome [12]. The liver was identified as the most frequent site of metastasis (30%-70% metastasis frequency), as well as the lung (20%-40%) and bone (5%-10%) [12]. To date, the prostate has only rarely been recognized as a confirmed site of colorectal metastases. It is often presumed to instead be a second primary cancer because of the large incidence (180,000/year) of prostate adenocarcinoma [13-16]. There is extensive literature describing the various metastatic sites of primary colorectal cancer, but rarely does research show involvement of the prostate, excluding second primary prostate adenocarcinoma. Presently, very few documented cases of prostate metastasis from primary colorectal cancer have been reported [17-21]. In this report, we present two rare cases of metastatic colon carcinoma in the prostate, thus adding to the small, yet growing body of reports describing this unusual site of involvement.
A review of the literature found only five reported cases for patients with colon cancer that had metastasized to the prostate. The first was diagnosed and reported in 1993, and the last in 2013 [17-21]. Additionally, to the best of our knowledge, this is the first case report of a male with metastatic breast cancer discovered in the kidney.
Case 1
A 73-year old male, with a history of glomerulosclerosis (diagnosed in 2004), underwent a failed right kidney transplant in 2012, and a successful left kidney transplant in 2013.
The patient was a smoker (20 pack-years (PY)) and had been treated appropriately for hypertension, hypothyroidism, ischemic heart disease and atrial fibrillation. He had a family history of a mother with colon cancer diagnosed at age 80, a sister with breast cancer diagnosed at age 50, and two nephews with lymphoma diagnosed at ages 8 and 15, respectively.
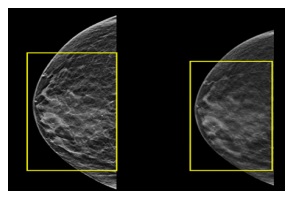
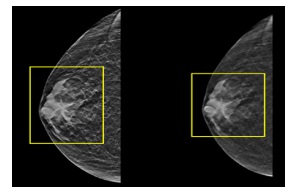
In November 2018, he underwent abdominal Computed Tomography (CT) due to complaints of hematuria, revealing a mass in the upper pole of the left (LT) kidney (4.7 X 5.4 cm). As part of further investigation, the patient underwent CT urography that confirmed the location of the mass in the upper pole of the left kidney, as well as blood clots in the renal pelvis and proximal urethra, bilateral pleural effusions, and traces of free fluid in the abdomen and pelvis. The patient underwent nephrectomy of the LT kidney due to suspected renal cell carcinoma. Histopathological analysis of the excised mass was highly suggestive of breast origin. Hormone receptor status was positive for estrogen and progesterone receptors, but negative for Human Epidermal Growth Factor Receptor 2 (HER-2). Ultrasound and mammography screening of the left breast showed prominent breast tissue throughout the breast (BIRADS 2), as well as prominent breast tissue in the right breast (BIRADS 2), suggestive of benign findings bilaterally. The patient subsequently underwent PET-CT, which did not reveal any areas of hypermetabolic activity. The patient is currently undergoing treatment with tamoxifen (Nolvadex) and his last PET-CT (November 2021) showed no evidence of any further metastatic disease.
Case 2
A 69-year old male patient with a history of hyperlipidemia, smoking (35 pack-years (PY)), and no family history of cancer, presented with abdominal pain and melena. In October 2015, he was diagnosed with colon adenocarcinoma T3 N2 M1 (stage 4) with peritoneal metastasis. In November 2015, the patient underwent left hemicolectomy with investigation and testing of a sub-diaphragmatic nodule. He began chemotherapy treatment under the FOLFOX protocol with added bevacizumab (Avastin). The regimen included bevacizumab 5 mg/kg, oxaliplatin 85 mg/m2 , leucovorin 400 mg/m2 and 5-FU 400 mg/m2 administered intravenously (IV) on day 1, followed by 5-FU 2400 mg/m2 IV continuous infusion over 46 hours every two weeks as adjuvant therapy for six cycles. One month after completing chemotherapy treatment, the patient underwent exploratory laparotomy and no malignancies were found.
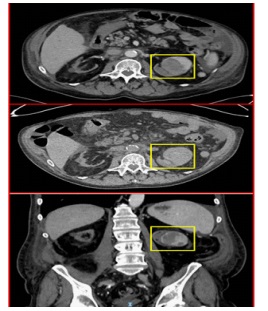
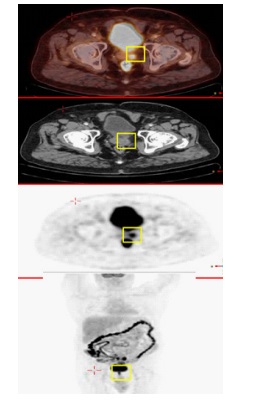
The patient was followed and 2 years later, in April 2017, PETCT showed areas of hypermetabolic uptake in the liver (1.7 cm in diameter), right colon, left iliac lymph-nodes and prostate.
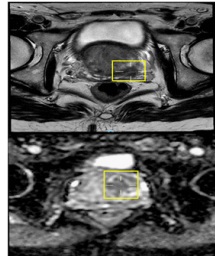
Upon further investigation, a second primary prostate cancer was suspected. As a result, Prostate-Specific Antigen (PSA) was analyzed and was found to be elevated with 6.2 ng/mL (normal 0 to 2.5 ng/mL). Magnetic Resonance Imaging (MRI) of the pelvis showed a mass over the seminal vesicle, and prostate cancer could therefore not be excluded. The patient underwent subsequent prostatectomy. Histopathological analysis showed adenocarcinoma of colonic origin. The patient is currently (December 2021) undergoing intermittent chemotherapeutic treatment
Case 3
A 73-year old male patient presented with a history of ischemic heart disease, diabetes mellitus, chronic kidney disease, hypertension and hyperlipidemia. He is a smoker (25 pack-years (PY)) and denied any family history of cancer. The patient complained of constipation and abdominal pain, inciting an investigative analysis. In September 2009, he was diagnosed with adenocarcinoma of the sigmoid colon with staging T3 N1 M0 (stage 3).
The patient underwent sigmoidectomy with negative surgical margins, and was treated with chemotherapy according to the FOLFOX protocol (oxaliplatin 85 mg/m2 , leucovorin 400 mg/ m2 and 5-FU 400 mg/m2 all administered IV on day 1, followed by 5-FU 2400 mg/m2 IV continuous infusion over 46 hours every two weeks) as adjuvant therapy for six cycles. In December 2014, PET-CT showed hypermetabolic uptake in the prostate area. In order to rule out a second primary of prostate cancer, PSA was taken and was found to be within normal limits (2 ng/ ml). The patient subsequently underwent prostatectomy, and histopathological analysis revealed adenocarcinoma of colonic origin. The patient is currently (December 2021) undergoing intermittent chemotherapeutic treatment.
Discussion & conclusion
Three cases of rare oncologic metastases were presented. The first patient was diagnosed with metastasis from male breast cancer that initially presented as a suspected renal cell carcinoma. Histopathology of the renal tissue confirmed a metastasis of breast tissue origin. The patient subsequently underwent a treatment protocol in accordance with the carcinoma’s hormonal status. The other two patients were diagnosed with colonic adenocarcinoma and the follow-up PET-CT demonstrated areas of hypermetabolic uptake in the prostate. Both cases were initially presumed to be second primary prostate cancers, but histopathology confirmed metastasis to the prostate originating from the colon. One of the patients initially refused prostatectomy and instead requested treatment according to prostate cancer protocol. However, after consideration, he agreed to surgical intervention. Although male breast cancer is known as a rare disease, the authors suggest that its metastases should be considered in various peripheral sites; including regions previously unsuspected and those recognized to have rare occurrences. In addition, it is important to further consider the possibility of rare metastases when assessing patients with prostate concerns suspicious for malignancy. Furthermore, a comprehensive investigation should be conducted when there are unusual findings to rule out any rare occurrences. Our review of the current literature yielded only five reported cases of patients with colon cancer with confirmed metastases to the prostate gland. The first was diagnosed in 1993, and the last was reported in 2013 (Table 1) [17-21]. To conclude, our reported case is the first to describe a male with metastatic breast cancer to the kidney. Additionally, we present two unique occurrences of metastases to the prostate that contribute to the growing body of literature describing less common metastatic findings.
Table 1:The basics of the previous reported cases for male patients with colon cancer that had metastasized to the prostate. ducts.
Reference No. |
Stage at presentation |
Age (years) |
Year of publication |
17 |
No Information Available |
No Information Available |
1993- February |
18 |
No Information Available |
No Information Available |
2002- August |
19 |
IIIC |
38 |
2004- May |
20 |
IIIC |
54 |
2011- June |
21 |
IV |
70 |
2013- June |

Acknowledgements: We would like to thank our patients that had agreed to share their stories and raise awareness for other patients and medical staff. In addition, we would thank our social worker Ms. Lena Turky for her help regarding to social conditions.
References
- Abdelwahab Yousef AJ. Male Breast Cancer: Epidemiology and Risk Factors. Seminars in oncology. 2017; 44: 267-272. https:// doi.org/10.1053/j.seminoncol.2017.11.002
- Burga AM, Fadare O, Lininger RA, et al. Invasive carcinomas of the male breast: A morphologic study of the distribution of histologic subtypes and metastatic patterns in 778 cases. Virchows Arch. 2006; 449: 507-512. https://doi.org/10.1007/s00428-006- 0305-3
- Anderson WF, Jatoi I, Tse J, & Rosenberg PS. Male breast cancer: A population-based comparison with female breast cancer. Journal of clinical oncology: Official journal of the American Society of Clinical Oncology. 2010; 28: 232-239. https://doi. org/10.1200/JCO.2009.23.8162
- Foerster R, Schroeder L, Foerster F, Wulff V, Schubotz B, Baaske D, et al. Metastatic male breast cancer: A retrospective cohort analysis. Breast care (Basel, Switzerland). 2014; 9: 267-271. https://doi.org/10.1159/000365953
- Zhou S, Yu B, Cheng Y, Xu X, Shui R, Bi R, et al. Zhonghuabing li xuezazhi = Chinese journal of pathology. 2014; 43: 231-235.
- Smymiotis V, Theodosopoulos T, Marinis A, Goula K, Psychogios J, Kondi-Pafiti A. Metastatic disease in the breast from nonmammary neoplasms. European journal of gynaecological oncology. 2005; 26: 547-550.
- Mandaliya H, Sung J, Hill J, Samali R, George M. Prostate Cancer: Cases of Rare Presentation and Rare Metastasis. Case reports in oncology. 2015; 8: 526-529. https://doi.org/10.1159/000442045
- Satram-Hoang S, Ziogas A, Anton-Culver H. Risk of second primary cancer in men with breast cancer. Breast cancer research: BCR. 2007; 9: R10. https://doi.org/10.1186/bcr1643
- Moot AR, Polglase A, Giles GG, Garson OM, Thursfield V, Gunter D, et al. Men with colorectal cancer are predisposed to prostate cancer. ANZ journal of surgery. 2003; 73: 289-293. https://doi. org/10.1046/j.1445-2197.2003.t01-1-02621.x
- Kim HS, Choi YJ, Shin DW, Han KD, Yoon H, Shin CM, et al. Secondary Primary Prostate Cancer after Colorectal Cancer: A Nationwide Population-based Cohort Study in Korea. Journal of cancer prevention. 2017; 22: 241-247. https://doi.org/10.15430/ JCP.2017.22.4.241
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A cancer journal for clinicians. 2018; 68: 394-424. https://doi. org/10.3322/caac.21492
- Stein U, Schlag PM. Clinical, Biological, and Molecular Aspects of Metastasis in Colorectal Cancer. In: Dietel M. (eds) Targeted Therapies in Cancer. Recent Results in Cancer Research. 2007; 176. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978- 3-540-46091-6_7
- Cancer Care. (2016, June). Treatment Update: Metastatic Prostate Cancer - Connect Booklet. https://www.cancercare.org/ publications/180-treatment_update_metastatic_prostate_cancer.
- Routh JC, Leibovich BC. Adenocarcinoma of the prostate: Epidemiological trends, screening, diagnosis, and surgical management of localized disease. Mayo Clinic proceedings. 2005; 80: 899-907. https://doi.org/10.4065/80.7.899
- Dulskas A, Cereska V, Zurauskas E, et al. Prostate cancer solitary metastasis to anal canal: Case report and review of literature. BMC Cancer. 2019; 19: 374. https://doi.org/10.1186/s12885- 019-5573-9
- Patel H, Kumar A, Shaaban H, Nguyen N, Baddoura W, et al. Synchronous metastasis of prostate adenocarcinoma to the stomach and colon: A case report. North American journal of medical sciences. 2014; 6: 152-154. https://doi. org/10.4103/1947-2714.128478
- Berman JR, Nunnemann RG, Broshears JR, Berman IR. Sigmoid colon carcinoma metastatic to prostate. Urology. 1993; 41:150- 152.
- Kang A, Lee JH, Lin E, Westerhoff M. Metastatic colon carcinoma to the prostate gland. Journal of computer assisted tomography. 2013; 37: 463-465. https://doi.org/10.1097/ RCT.0b013e3182898248
- Youssef FR, Hunt L, Meiring PD, et al. Metastasis of a cecal adenocarcinoma to the prostate five years after a right hemicolectomy: A case report. J Med Case Reports. 2011; 5: 223. https:// doi.org/10.1186/1752-1947-5-223
- Gupta T, Laskar SG, Thakur M, Desai S, Shrivastava SK, et al. Isolated prostatic metastasis from primary sigmoid colon carcinoma. Indian journal of gastroenterology: Official journal of the Indian Society of Gastroenterology. 2004; 23: 114-115.
- Schips L, Zigeuner RE, Langner C, Mayer R, Pummer K, et al. Metastasis of an ascending colon carcinoma in the prostate 10 years after hemicolectomy. The Journal of urology. 2002; 168: 641-642.