
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Skeletal deformities in a case of digitocutaneous dysplasia
Vij N1; Belthur MV2*
1University of Arizona College of Medicine, 475 N 5th St., Phoenix, AZ 85004, USA.
2Phoenix Children’s Hospital, Department of Orthopedics, Main Building, Clinic B, 1919 E Thomas Rd, Phoenix, AZ 85016, USA.
*Corresponding Author: Mohan V Belthur
Phoenix Children’s Hospital, Department of
Orthopedics, Main Building, Clinic B, 1919 E Thomas
Rd, Phoenix, AZ 85016, USA.
Tel: 602-934-1660, Fax: 602-933-5245;
Email: mvbelthur@yahoo.com
Received : Dec 14, 2021
Accepted : Jan 21, 2022
Published : Jan 28, 2022
Archived : www.jcimcr.org
Copyright : © Belthur MV (2022)
Keywords: fibromatosis; bone tumors; skeletal dysplasias; multidisciplinary care.
Citation: Vij N, Belthur MV. Skeletal deformities in a case of digitocutaneous dysplasia. J Clin Images Med Case Rep. 2022; 3(1): 1623.
Description
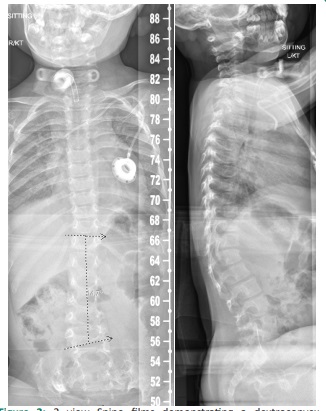
We present a case of a 2 year old female with digital fibrous lesions, dysmorphic facial features, stridor, sensorineural hearing loss, and scoliosis. The patient surgical history included digital amputations at the interphalangeal joint line bilaterally on the middle, ring, and little finger. Physical exam demonstrated knee and elbow flexion contractures and a left ankle varus contracture. Radiographic evaluation revealed several aggressive fibromas in the proximal femori and tibia (Figure 1) and a mild dextroconvex lumbar scoliosis (Figure 2) [1,2]. Biopsy of a digital lesions revealed a dermal spindle cell proliferation without atypia or necrosis, and perinuclear inclusions on H&E and trichrome stains. Comparative genomic hybridization and single nucleotide polymorphism genotyping revealed two adjacent duplications of the DMD gene (OMIM 400477): a duplication of 83 kb from the cytogenic band Xp21.2 to Xp 21.1 and a duplication of 555 kb within the cytogenetic band of Xp21.2.
The patient was subsequently followed in the orthopedic clinic, ENT clinic, and dermatology clinic. Due to large laryngeal tumor-like masses that caused progressive dyspnea, apnea, and stridor, the patient required a tracheostomy and dilatation of subglottic stenosis. Serial radiographs of the spine revealed progression of the curve with development of thoracolumbar junction kyphosis and lumbar lordosis. Due to the patients’ age, underlying osteopenia, and complexity of her case, thoracolumbar sacral bracing and physical therapy were chosen as the preferred treatment. Our case demonstrates two teaching points. Firstly, biopsy and genetic testing in digitocutaneous dysplasia can be vague [3-5] and often times a clinical diagnosis based on presentation and radiography is required. Secondly, the decision not to operate in young infants with Digitocutaneous dysplasia may be right to reduce unnecessary surgeries. If aligned with the patient’s and families goals, a definitive spinal fusion could always be sought out at skeletal maturity.


Final diagnosis: Digitocutaneous dysplasia
Three differential diagnosis:
1. Metaphyseal Epiphyseal Dysplasia
2. Diastrophic Dysplasia
3. Kniest Dysplasia
References
- Panda A. Skeletal dysplasias: A radiographic approach and review of common non-lethal skeletal dysplasias. World J Radiol. 2014; 6(10).
- Beals RK, Horton W. Skeletal Dysplasias: An Approach to Diagnosis. J Am Acad Orthop Surg. 1995; 3(3).
- Hinton VJ, Cyrulnik SE, Fee RJ, Batchelder A, Kiefel JM, Goldstein EM, Kaufmann P, De Vivo DC. Association of Autistic Spectrum Disorders With Dystrophinopathies. Pediatr Neurol. 2009; 41(5).
- Darras BT, Menache-Starobinski CC, Hinton V, Kunkel LM. Dystrophinopathies. In: Neuromuscular Disorders of Infancy, Childhood, and Adolescence: A Clinician’s Approach. 2015.
- Stenson PD, Mort M, Ball E V, Shaw K, Phillips AD, Cooper DN. The Human Gene Mutation Database: Building a comprehensive mutation repository for clinical and molecular genetics, diagnostic testing and personalized genomic medicine. Human Genetics. 2014; 133.