
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
What can reveal occipital growth in newborns? Meningo-encephalocele
Oze K Rita; Yehouenou Tessi Romeo Thierry*; El Haddad Siham; Allali Nazik; Chat Latifa
Radiology Department, Ibn Sina Paediatric Teaching Hospital, Mohammed V University, Rabat, Morocco.
*Corresponding Author: Yehouenou Tessi Romeo
Thierry
Department of Radiology, Ibn Sina Paediatric Teaching
Hospital, Mohammed V University, Rabat, Morocco.
Tel: + 212-613211125;
Email: nactessi@yahoo.fr
Received : Dec 06, 2021
Accepted : Jan 24, 2022
Published : Jan 31, 2022
Archived : www.jcimcr.org
Copyright : © Thierry YTR (2022).
Keywords: occipital growth; congenital anomaly; brain CT; méningo-encephalocele.
Citation: Oze KR, Yehouenou Tessi RT, El Haddad S, Allali N, Chat L. What can reveal occipital growth in newborns? Meningo-encephalocele. J Clin Images Med Case Rep. 2022; 3(1): 1625.
Description
The occipital encephalocele is a rare homozygous congenital malformation, linked to the C677T gene according to Molloy et al [1,2]. In relation to a defect in the closure of the cranial part of the neural tube during intrauterine life, it is therefore defined such as a hernia of the nervous tissue (part of the cerebellum) and / or the meninges through a bone defect in the occipital region. Its incidence is 0.8 to 3.0 per 10,000 births (sex ratio of 0 girls to 9 boys) according to some studies. It can be meningocele (only meninges), encephalocele (only brain tissue) or meningoencephalocele (brain tissue and meninges). Etiologically, several factors have been implicated in their occurrence. According to Lemire and Robert L, these factors act for some malformations during neurilation, i.e., between the first 30 days of gestation and the closure of the posterior neuropore, and for others in the post-neurilation period. Young maternal age and multiparity are also associated with neural tube defects. Clinically, it varies in size ranging from a small tumefaction or even a large painless mole mass covered with skin tissue [1-3].
Currently, the only effective treatment for encephaloceles is reconstructive surgery, usually performed in infancy. Imaging being essential for the diagnosis, it is contributory prenatal through ultrasound as a purely cystic mass or with echoes of herniated brain tissue. It may be a solid mass in case of encephalocele. Postnatal cross-sectional cerebrospinal imaging with high-resolution CT makes it possible to display the bone anatomy. MRI being the best imaging modality to define the content of an encephalocele before any surgery, it better defines the intracranial connection [4].
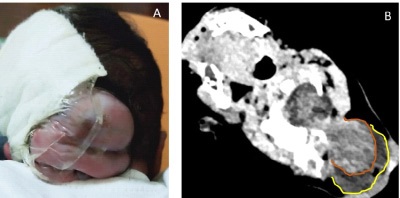
This is the case of the male newborn baby, Apgar 9/10/10, eupneic, presenting an occipital growth (Figure 1A). Non-injected brain scan has been done to explore this occipital mass.
The cerebral CT scan not injected in multi planar reproduction made it possible to show in axial section (Figure 1 B), showing a median occipital bone defect through which protrudes an oval sac made of meningeal envelopes (yellow curve), brain tissue (brown curve).
Conflicts of interest: The authors declare that they have no conflicts of interest.
References
- Rowland CA, Correa A, Cragan JD, Alverson CJ. Are encephaloceles neural tube defects? Pediatrics. 2006; 118: 916-923.
- Sanoussi S, Chaibou M, Bawa M, Kelani A, Rabiou M, et al. Encéphalocèle occipitale: Aspects épidémiologiques, cliniques et thérapeutiques: A propos de 161 cas opérés en 9 ans à l’hôpital national de niamey. African Journal of Neurological Sciences. 2009; 28.
- Messaoud MB, Khalfaoui S, Darmoul M, Kilani M, Hattab MN. Encéphalocèle occipitale à propos de 20 cas. Neurochirurgie. 2018; 64: 270.
- Morón FE, Morriss MC, Jones JJ, et al. Bosses et bosses sur la tête chez les enfants: Utilisation de l’imagerie CT et IRM pour résoudre le dilemme du diagnostic clinique. Radiographie. 24: 1655-1674.