
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Benign prostatic-type epithelium polyp presenting as a progressive mass in young adult: Case report
Nada Shaker1; Ankush Patel2; Nuha Shaker3; Anil Parwani4*
1 PGY-1 Resident, Department of Pathology, The Ohio State University Wexner Medical Center, Columbus, OH, USA.
2 The Ohio State University Wexner Medical Center, Columbus, OH, USA.
3 PGY-3 Resident, Department of Pathology, The University of Kentucky, Lexington, KY, USA.
4 Vice Chair and Director, Anatomic Pathology, Department of Pathology, The Ohio State University Wexner Medical Center, Columbus, OH, USA.
*Corresponding Author: Anil Parwani
Professor of Pathology and Biomedical Informatics,
Vice-Chair of Anatomic Pathology, Director of
Pathology Informatics Director, Digital Pathology
Shared Resources, Principal Investigator, Cooperative
Human Tissue Network (CHTN) Midwestern Division
Wexner Medical Center - Department of Pathology,
The Ohio State University, E409 Doan Hall, 410 West
10th Ave, Columbus, OH, 43210, USA
Email: anil.parwani@osumc.edu
Received : Nov 11, 2021
Accepted : Jan 27, 2022
Published : Feb 03, 2022
Archived : www.jcimcr.org
Copyright : © Parwani A (2022).
Citation: Shaker N, Patel A, Shaker N, Parwani N. Benign prostatic-type epithelium polyp presenting as a progressive mass in young adult: Case report. J Clin Images Med Case Rep. 2022; 3(2): 1633.
Introduction
Our report details the clinically significant presentation of a large non neoplastic prostatic-type polyp found in a 37-year-old male patient seeking management for a pelvic mass involving the seminal vesicles and prostate. Prostatictype polyps uncommonly present within the urothelial tract, with the majority arising within the prostatic urethra in and around the verumontanum and less commonly within the bladder [1-3]. Epidemiology is broad, with an affected range spanning 19-89 years of age, though suggested to be more common in elderly patients with benign prostatic hyperplasia [3,4]. Etiological origins of metaplastic or hyperplastic changes, abnormal migration and misplacement of prostatic tissue, and the persistence of embryonic remnants have been suggested, however histogenesis may vary depending on the site of the polyp [3-6]. Our case depicts a unique presentation of prostatic-type polyp of the urothelial tract distinctive in gross appearance, histological findings, clinical evaluation, course, and management.
Case presentation
A 37-year-old male presenting to The Ohio State University for evaluation of a three-year duration of intermittent, painless, gross hematuria accompanied by initial episodes of hematospermia prompted a CT urogram investigation indicating a 7.2 cm lobulated ill-defined mass arising from the seminal vesicles. Persistent mass was identified on CT pelvis following a two-week treatment regimen of Levaquin and Prednisone. A benign lesion was shown on subsequent prostate and seminal vesicle biopsy.
Mass effect symptoms of decreased urinary flow, weak urinary stream, and hesitancy spurred Transurethral Resection of the Bladder Mass (TURP), demonstrating predominantly necrotic and calcified tissue fragments without malignancy.
The patient declined suggested surgical removal of the mass citing associated procedural side effects and the benign nature of the lesion. Follow-up with primary care physician was continued with prostate MRI every 3-6 months, demonstrating an increase in mass size for 1.5 years following TURP. During this time, the patient experienced once daily and once nightly episodes of urinary incontinence with no associated preceding symptoms or specific triggering events. Symptoms of sexual dysfunction proceeding resection, e.g., erectile dysfunction and infertility, were denied by the patient, who reported conceiving a son following the procedure. A short course of oxybutynin was implemented after TURP to mitigate the potential of bladder spasms as a cause for incontinence, however the patient reported no improvement.
Notable symptomatic progression of constipation, voiding difficulty, urinary urgency, incontinence, and frequency accompanied the last 6 to 8 months of increasing mass size following resection, with severe paucity of urinary flow preventing orthostatic urination. Significant straining occurred during urinary and bowel excretion, with the patient noting feelings of incomplete evacuation. Urinary urgency progressed to episodes of nocturia occurring four to five times per night.
Repeat MRI imaging at this time demonstrated a lesion diameter approaching 11.4 cm, with encroaching proximity upon the sacral nerves and planar loss between the lesion and prostate presenting concerns of limited resectability potential. The patient ultimately underwent robotic cystoprostatectomy after progressive severity of hematuria and urinary incontinence. Symptoms of sexual dysfunction, hematuria, and fatigue from nocturia were noted following procedure, with the patient reporting the inability to conceive after attempting to do so for six months. The patient denied any history of STIs, abdominal pain, nausea or vomiting, shortness of breath, chest pain, new bone pain, visual changes, night sweats, flank pain, weight loss or weight gain following cystoprostatectomy.
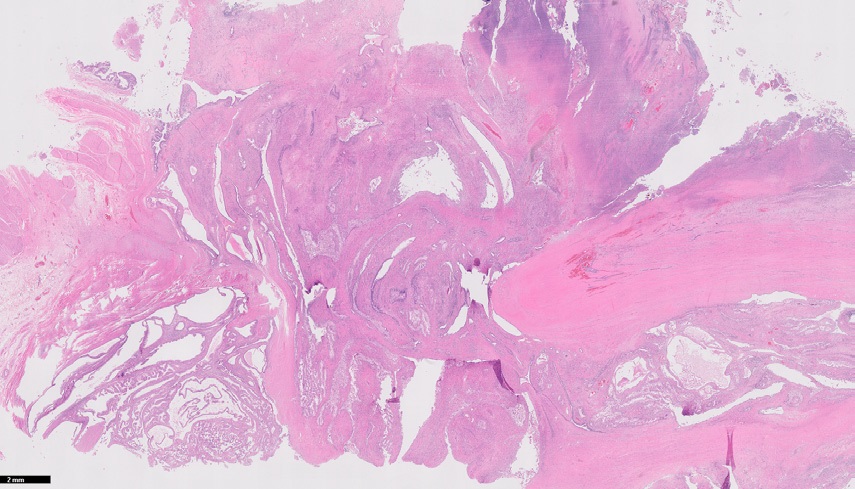
On gross examination of the pelvic mass (prostate, seminal vesicles, and bladder), a large nodular mass causing distortion of the prostate gland was seen. Total glandular measurements were recorded: 11.5 cm (right to left) X 6.9 (apex to base) X 7.5 cm (anterior to posterior).
Opening of the specimen revealed a 9.2 X 7.1 X 7.5 cm diffusely cystic, diffusely necrotic mass appearing to arise from the right half of the prostate. The mass appeared to border upon the distal urethral/prostatic apex margin, extending to the bladder mucosa and muscularis on the right lateral bladder wall, though not into the peri-vesicular fat. The remainder of the bladder mucosa was gray-brown and slightly edematous with no additional lesions. The mass bordered the inked outer surface on both the right anterior lateral and posterior aspects of the bladder. It also appeared to involve the right seminal vesicle, abutting, though not grossly involving the right vas deferens. The mass remained 0.7 cm from the posterior inked outer surface of the bladder. Sectioning through the uninvolved prostate revealed pale tan-pink, diffusely fibrotic cut surfaces. There was no uninvolved prostate gland or seminal vesicle identified in the right half. No palpable lymph nodes were identified in the peri-vesicular fat.
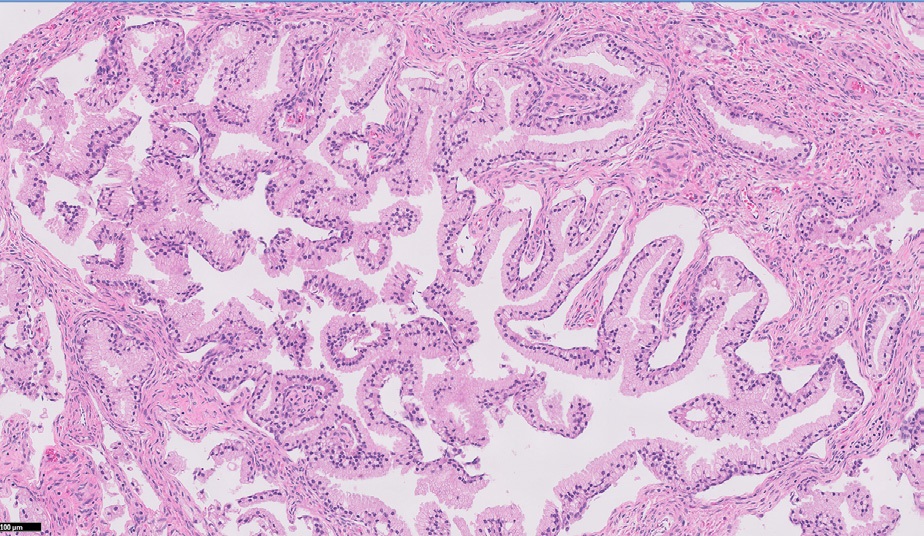
Microscopic examination of the mass exhibited a large, mostly necrotic benign polypoid epithelial “polyp”/mass with prostatic type epithelium, with a cystic growth pattern. The neoplasm, including the necrotic areas, measured 9.2 cm in greatest dimension. The mass appeared to arise from the prostatic urothelium and into the bladder mucosa, with additional involvement of the right seminal vesicle area. Extensive acute and chronic inflammation of the bladder wall surrounding the necrotic areas was also noted (Figure 1,2). All margins were negative for cancer.
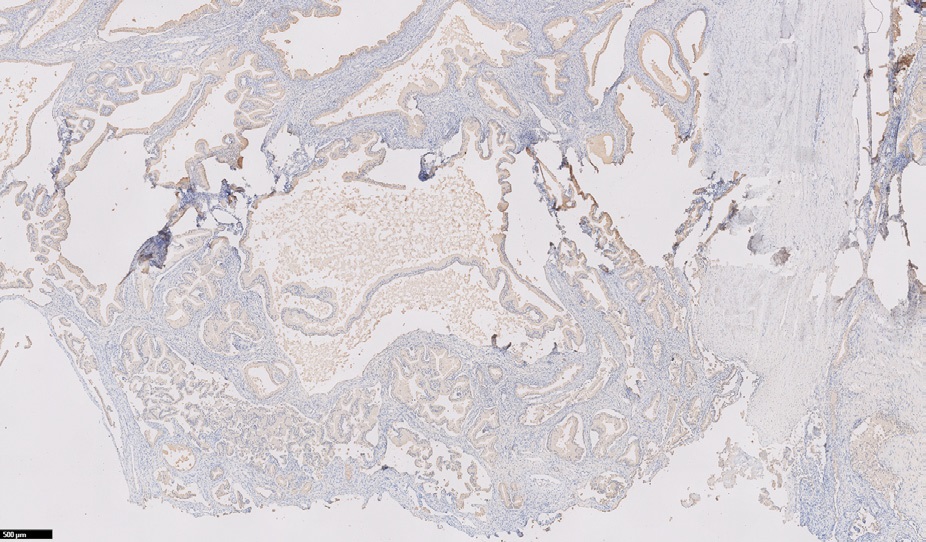
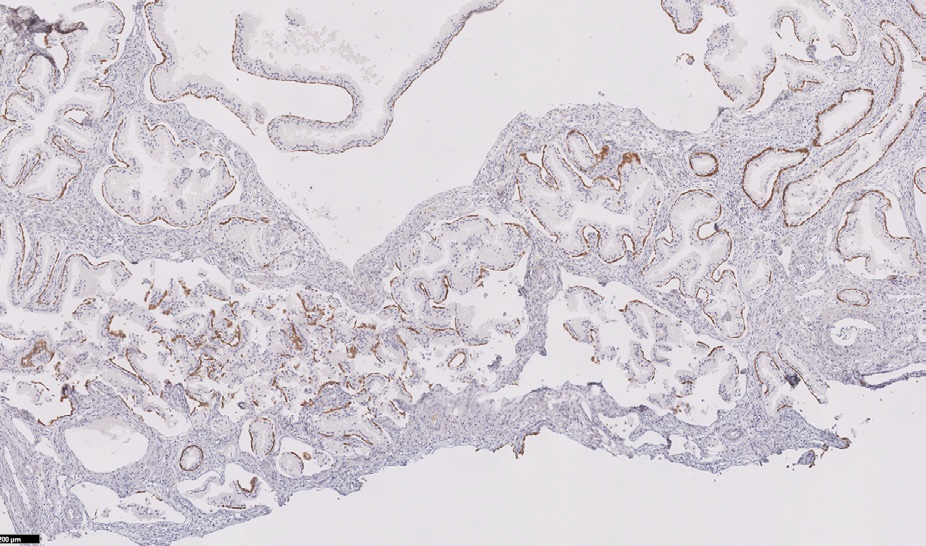
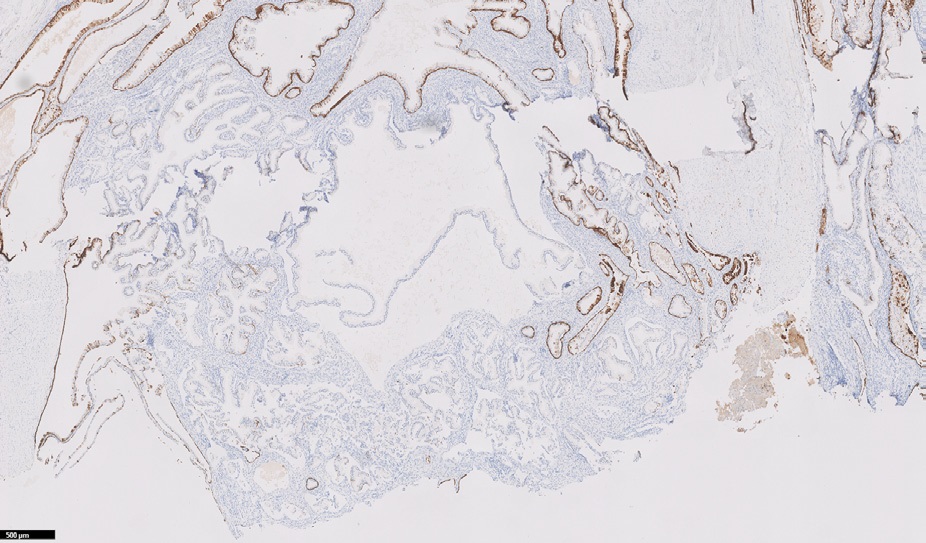
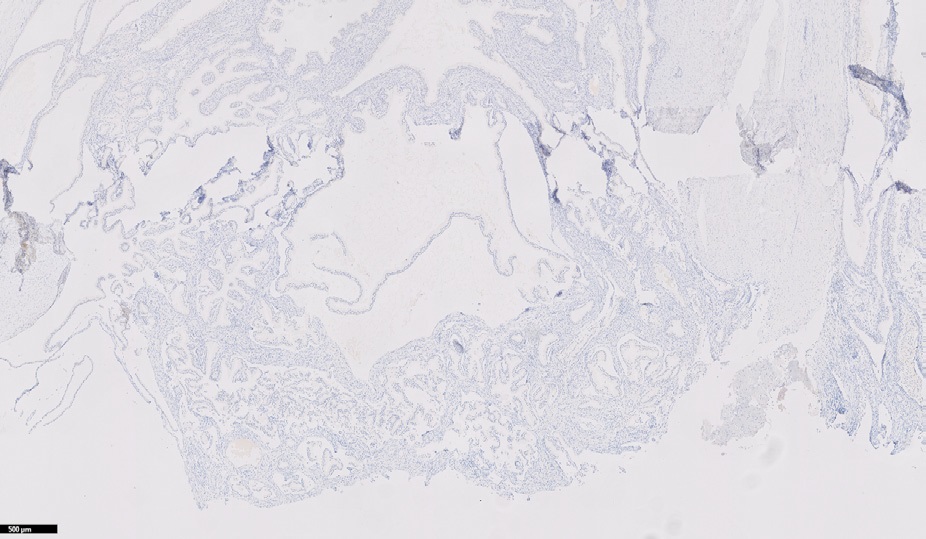
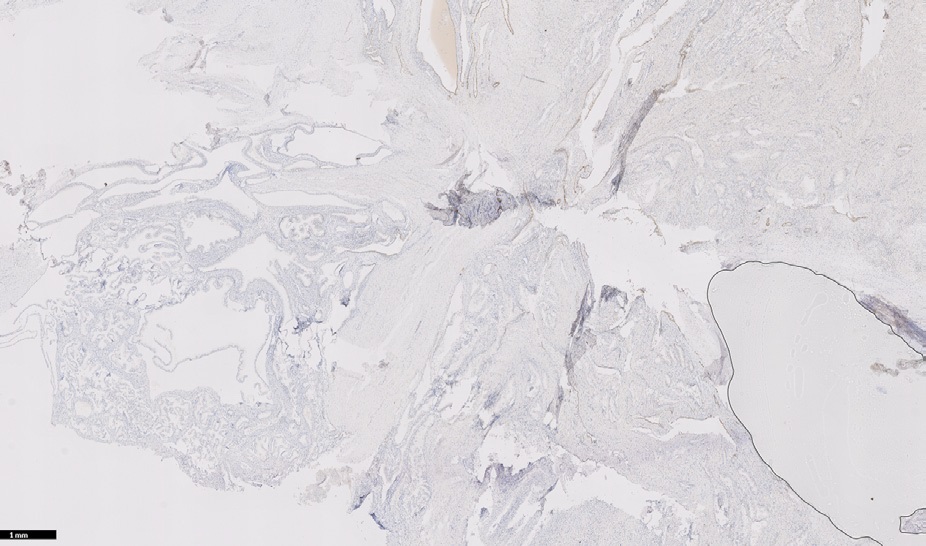
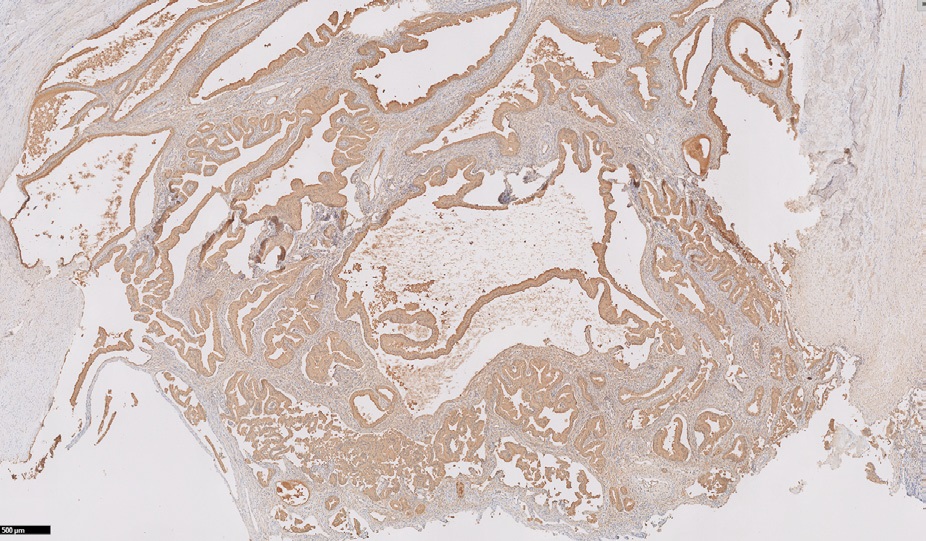
Immunohistochemical staining performed at The Ohio State University was positive for PSAP, PSA, NKX3.1, p63, CK903, and negative for GATA3, CK7, AMACR, and CK20. Figure 3-9. GATA3 and CK7 were only positive within the urothelial lining.
Following cystoprostatectomy, the patient underwent neobladder reconstruction. A regimen of Viagra (Sildenafil) and Bi-Mix (Papaverine HCl 30 mg/mL, Phentolamine Mesylate) was implemented for erection control. Mild night time incontinence with negative daytime incontinence, pelvic, or flank pain was noted after one year follow-up.

Discussion
Prostatic-type epithelial polyps were first described approximately 100 years ago [3]. Since then, such lesions have been uncommonly found within the urinary tract, often forming on the posterior urethra [3]. The minority of lesions found in the bladder are most commonly located in the trigone. To the best of our knowledge, our case report is only the second featured within the literature to include involvement of the right lateral bladder wall [3].
At the time of this publication, there have been no reports of prostatic-type epithelial polypoid involvement of the seminal vesicles. Heterogenous enlargement of the right seminal vesicle, extending into the level of the adjacent prostate gland was noted in our patient. We believe this finding to be likely indicative of a primary lesion of the seminal vesicle.
In diagnostic evaluation of prostatic-type polypoid urothelial lesion, great consideration must be given to prostatic ductal adenocarcinoma. This vital differential for exclusion typically contains a comparatively enhanced architectural complexity of cribriform and anastomosing cords, pseudostratified columnar epithelium, and prominent nucleoli belying low-grade nuclear features. Immunohistochemical staining of prostatic ductal adenocarcinoma is similarly positive for PSA and PAP / PSAP.
Prostatic type epithelial polyps of the urothelial tract are typically first identified on transrectal ultrasonography, demonstrating a homogenous isoechogenicity similar to that seen in the bladder wall [7]. Diagnosis is then confirmed by cystoscopy with biopsy or transurethral resection of the prostate with subsequent histological examination of tissue. The exceptionally large nature of the mass presented in our case was initially discovered on CT urogram following an episode of hematospermia, prompting further investigation with pelvic CT.
Several other differential diagnosesmay be taken into consideration during evaluation of a prostatic-type lesion of the urothelium. Urothelial carcinoma with glandular differentiation consists of pseudostratified columnar epithelium lining the glands with cytologic atypia of urothelial and glandular components. CK7 and GATA3 staining are positive only within the urothelial component of this differential. Papillary urothelial neoplasms must also be differentiated from prostatic-type polyps of the epithelium. Morphology here includes papillary architecture with secondary or tertiary branching with stratified epithelium and no glandular component. Staining is positive for CK7 and GATA3. Benign Prostatic Hyperplasia (BPH) contains varying amounts of benign prostatic glands and spindle cells and may be mistaken for a prostatic-type urothelial polyp due to the potential to form a polypoid mass which may protrude into the bladder area near the anatomical neck. Nephrogenic adenoma also must be considered in differential assessment, as it contains a single layer of cuboidal epithelial cells and morphology of varying patterns including a combination of papillary and polypoid with tubules in the underlying stroma. Staining is positive for PAX8, CK7, and AMACR, with PSA or PAP demonstrating occasional weak positivity. The architecture of polypoid or papillary cystitis may mimic that of urothelial prostatic-like polyp and may be distinguished by absence of prostatic glandular epithelium and corpora amylacea, as well as negative immunohistochemistry staining for PSA and PAP. The absence of these morphological elements in conjunction with negative staining for PSA and PAP is also distinctive of cystitis cystica and cystitis glandularis, conditions which also must be considered due to their polypoid appearance. They are identified by cystic and gland-like strucutres of varying size and shape lined by urothelium.
Gross appearance of urothelial prostatic-like polyps typically reveals small polypoid or papillary lesions, with histology demonstrating nonneoplastic prostatic-type glandular epithelium within the stroma [1,4,8]. Associated clinical symptoms include gross or microscopic hematuria, hematospermia, dysuria, and urinary outflow obstruction [1,3,4]. Simple resection is often curative, with prognosis of typically favorable due to the low potential for recurrence afforded by its nonneoplastic nature [1-3,5]. Resection with TURP was ineffective in our patient, with recurrence of the mass and exacerbation of mass-effect symptoms prompting cystaprostatectomy
References
- Anjum MI, Ahmed M, Shrotri N, Azzopardi A, Mufti GR. Benign polyps with prostatic type epithelium of the urethra and the urinary bladder. Int Urol Nephrol. 1997; 29: 313-317.
- Halat S, Eble JN, Grignon DJ, et al. Ectopic prostatic tissue: Histogenesis and histopathological characteristics. Histopathology. 2011; 58: 750-758.
- Zhu H, Lin Y, Wang B, Shen B, Xie L. Prostatic-type polyp located in the bladder of an adolescent: A case report and overview. J Int Med Res. 2019; 47: 1787-1792.
- Chan JK, Chow TC, Tsui MS. Prostatic-type polyps of the lower urinary tract: Three histogenetic types? Histopathology. 1987; 11: 789-801.
- Bellezza G, Sidoni A, Cavaliere A. Ectopic prostatic tissue in the bladder. Int J Urol. 2005; 12: 1066-1068.
- Ishikawa J, Yasuno H, Higuchi A, Kamidono S, Okada S. Benign polyp with prostatic-type epithelium of the urinary bladder: A case report. Hinyokika Kiyo. 1990; 36: 1463-1465.
- Ko SY, Kim YJ, Park HS, et al. Sonographic findings of ectopic prostatic tissue in the bladder: A case report and review of the literature. Clin Imaging. 2013; 37: 778-779.
- Remick DG, Jr, Kumar NB. Benign polyps with prostatic-type epithelium of the urethra and the urinary bladder. A suggestion of histogenesis based on histologic and immunohistochemical studies. Am J Surg Pathol. 1984; 8: 833-839.