
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Spontaneous uterine rupture at 31 weeks of amenorrhea on unscarred uterus: Case report
Saloua Tanouti1,2,3*; Hafsa Taheri1,2,3; Hanane Saadi1,2,3; Ahmed Mimouni1,2,3
1 Department of Obstetrics and Gynecology, Mohammed VI University Hospital Oujda, Morocco.
2 Department of Obstetrics and Gynecology, Faculty of Medicine Oujda, Morocco.
3 Department of Obstetrics and Gynecology, Mohammed First University Oujda, Morocco.
*Corresponding Author: Tanouti Saloua
Department of Obstetrics and Gynecology, Mohammed VI University Hospital Center, Oujda, Morroco.
Address: Morocco, BP 6527, Rabat, Morocco.
Email: saloua.tanouti@gmail.com
Received : Dec 13, 2021
Accepted : Jan 28, 2022
Published : Feb 04, 2022
Archived : www.jcimcr.org
Copyright : © Saloua T (2022).
Abstract
Uterine rupture in pregnancy is associated with severe maternal and fetal complications. Although it is a rare event, uterine rupture has been associated with certain risk factors.
We present the case of a 30-year-old parturient fourth gesture, third par, all delivered vaginally admited to the emergency room for spontaneous uterine rupture in a non-scarred uterus at 31 weeks of amenorrhea revealed by an a typical misleading digestive symptoms, the patient was immediately operated and put in intensive care unit postoperatively with good maternal and fetal evolution.
Uterine rupture in a non-scarring uterusis a rare, unpredictable and serious complication.
Citation: Tanouti S, Taheri H, Saadi H, Mimouni A. Spontaneous uterine rupture at 31 weeks of amenorrhea on unscarred uterus: Case report. J Clin Images Med Case Rep. 2022; 3(2): 1636.
Introduction
Uterine rupture during pregnancy is a serious condition associated with high maternal-fetal morbidity and mortality [1]. Few researchers have reported spontaneous uterine rupture without underlying causes, regardless of the gestational age or multiparous status. The rupture of an unscarred uterus has been reported to occur in 1 out of 15,000 cases [2].
Here we report the case of a 30-year-old parturient who presented with spontaneous uterine rupture in a non-scarred uterus at 32 weeks of amenorrhea, which was revealed by a typical misleading digestive symptoms. In the following, we discuss the diagnosis and treatment. Further more, we compare the presentation of our patient to the findings of previous studies.
Case presentation
We report the case of a 30-year-old parturient, gestation 4, para 3, all delivered vaginally, and without instrumental maneuvers. The gestational age of the current pregnancy was estimated at 31 weeks of amenorrhea. This pregnancy was well monitored, with two ultrasounds performed at 12 weeks, and 22 weeks of amenorrhea. At 31 weeks of amenorrhea, the parturient was admitted to the emergency room for diffuse and intense abdominal pain with vomiting and diarrhea.
On admission, physical examination revealed a conscious patient who was stable hemodynamically and respiratory, with a blood pressure of 110 mmhg/60 mmhg and a heart rate of 90 bpm with no fiver.
Gyneco-obstetrical examination revealed diffuse abdominal tenderness with abdominal distention. Fetal heart sounds were perceived, and no uterine contracture was found. Vaginal examination revealed a posterior cervix with no dilatation or effacement. The fetal presentation was mobile cephalic, and the amniotic sac was intact, with no per vaginal bleeding.
Obstetric ultrasound revealed a progressive monofetal pregnancy with an estimated fetal weight of 1600 g, corresponding to the 50th percentile. The quantity of amniotic fluid was adequate, with the placenta posterior, fundal, and lateralized to the left. There was peritoneal effusion of average abundance.
The fetal heart rate registration was normal. Laboratory investigations revealed microcytic hypochromic anemia with hemoglobin of 8.1 g/dl, no thrombocytopenia, a platelet count of 225000 Lmm3 , a correct prothrombin ratio of 97%, fibrinogen 2.5, and blood type ARH+.
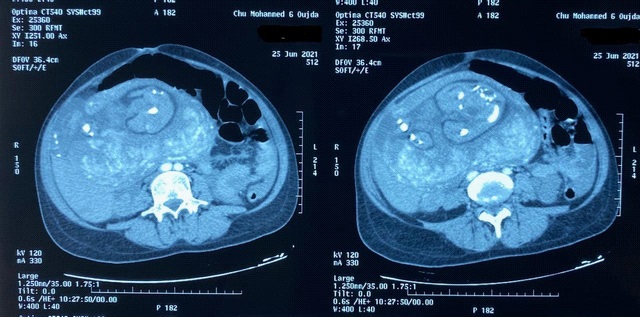
Because of the presence of a peritoneal effusion on ultrasound examination and the vomiting, an abdomino pelvic scan was performed, revealing a large uterine rupture with extravasation of the contrast medium from the uterine fund us and a hemoperitoneum of great abundance (Figure 1).
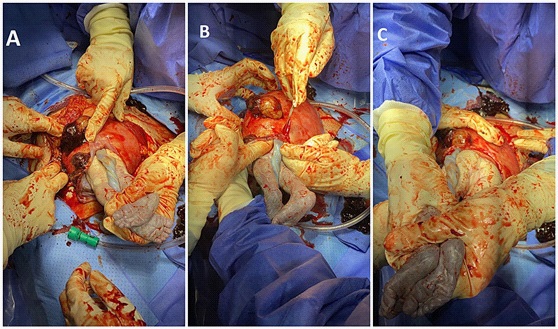
The patient was rushed to the operating room and put under general anesthesia. A Pfannenstiel-type incision was made. Intraoperatively, there was a large hemoperitoneum made of darkred coagulated blood, and it was aspirated. There were a rupture at the level of the uterine fund us Measured 5 cm long, was lateralized to the right, with the protruding amniotic sac blocking the rupture (Figure 2).
An amniotomy of the protruding amniotic sac was made followed by a podalic extraction after enlarging the rupture using a scalpel. A female infant with an APGAR score of 7/10 at the first minute, then 9/10 at the fifth minute, was born, with a birth weight of 1700 g, and was hospitalized in neonatology unit for respiratory distress, benefiting from a surfactant cure with a good development there after.
The fundal rupture was sutured in two layers with a number 2 vicryl (Figure 3).
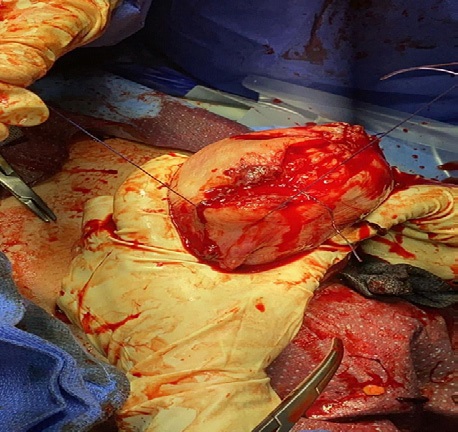
We had a good safety globe with good hemostasis control. A bilateral tub alligation was performed.
The patient was hospitalized in the mother-child intensive care unit, where she was transfused by one unit of red blood cells with a good postoperative outcome.
The patient was transferred to the obstetrics and gynecology department after a 48-hour stay in intensive care.
Discussion
Imaging features of HCC on MRI
Uterine rupture is a solution of complete continuity of the uterine wall, as well as the adjacent peritoneal layer, which can occur spontaneously in 25% of cases or could be traumatic, following a shock, an obstetric, or an instrumental maneuver [3,4]. It is rare in developed countries, occurring in 1/2000 births, while its incidence is much higher in developing countries, occurring in approximately 1/100 births [4].
The majority of published rupture cases occurred at the end of pregnancy or during labor, and 17% appeared before the on set of labor [5,3]. The location of the rupture can be lower segmental (during labor), or bodily (for ruptures occurring outside of labor) [1]. There are many predictors of uterine rupture, the most important of which are scarred uterus, malformed uterus, multiparity, obstetric maneuvers, instrumental extractions, mechanical obstructions, history of uterine curettage, and the use of oxytocinanalogs [5]. The typical signs of uterine rupture are severepelvic pain, a tearing sensation, bleeding, and unstable hemodynamics progressing to shock [6,3].
The peculiarity of ourclinical case is in the absence of predisposing or predictive factors in the associated digestive picture and the absence of metrorrhagia with a stable hemodynamic state.
A study carried out in 2004 reported aperinatal mortality rate ranging from 18.5% to 26.9% in patients with healthy and scarred uterus, concluding that there was no statistically significant difference between the two groups. The same conclusion was reached regarding maternal mortality [5].
In our patient, the paucity of clinical signs that led to this unrecognized rupture can be explained by the fact that the broad ligament remained intact, playing a compressive role, and the protruding amniotic pouch blocked the rupture. Since the clinical picture is misleading, CT scanning played an important role in the diagnostic process.
The recommended management requires a first intensive resuscitation followed by surgical treatment, ideally consisting of a conservative approach in young women wishing to become pregnant, and it involves simple suturing of the rupture. When conservative treatment seems impossible due to the extent of lesions, a hysterectomy is required [7,8]. In our case, the patient consented to tuballigation.
The main obstetric differential diagnoses to be considered urgently are retro placental hematoma with or without associated HELLP syndrome or a detachment of the normally inserted placenta for which imaging may be beneficial [9,3].
The risk of recurrence in the event of a new pregnancy ranges from 4% to 19%, depending on many series [1,5]. Therefore, it is necessary to fully inform the patient and to ensure her understanding to establish effective contraception and avoid any unwanted pregnancies [10].
Most authors agree that the risk of recurrence is higher on a scar on the body than on a scar in the lower segment, estimated to range from 4% to 9% in the first case, and from 0.2% to 1.5% in the second [11], which explains our decision to perform a tubal ligation.
Conclusion
Uterine rupture in an unscarred uterusis a rare, unpredictable, and serious complication. It should be considered in all pregnan two men experiencing abdominal pain and signs of peritoneal irritation, regardless of the gestational age and history. Its diagnosisis mainly based on imaging as the clinical picture can sometimes be poor or misleading. The management of this incident is a vital emergency involving the maternal and fetal prognosis, as well as the obstetrical outcome for the patient.
References
- Zeteroğlu S, Aslan M, Akar B, Bender RA, Başbuğ A, et al. Uterine rupture in pregnancy subsequent to hysteroscopic surgery: A case series. Turkish. J Obstetr Gynecol. 2017; 14: 10-4274.
- Park YJ, Ryu K, Lee JI, Park MI. Spontaneous uterine rupture in the first trimester: A case report. J. Korean Med Sci. 2005; 20: 1079-1081.
- Bretones S, Cousin C, Gualandi M, Mellier G: Rupture uterine. J Gynecol Obstet Biol Reprod. 1997; 26: 324-327.
- Catanzarite V, Cousins L, Dowling D, Daneshmand S. Oxytocin associated rupture of an unscarred uterus in a primigravida. Obstet Gynecol. 2006; 108: 723-725.
- Wang YL, Su T. Obstetricuterine rupture of the unscarred uterus: A twenty-year clinical analysis. Gynecol Obstet Invest. 2006; 62: 131-135.
- Mazzone ME, Woolever J. Uterine rupture in a patient with an unscarred uterus: A case study. WMJ. 2006; 105: 64-66.
- Fatfouta I, Villeroy de Galhau S, Dietsch J, Eicher E, Perrin D, et al. Rupture utérine spontanée sur utérus sain pendant le travail: À propos d’un caset revue de la littérature: Gynecol Obstet Biol Reprod. 2008; 37: 200-203.
- Leung F, Courtois L, Aouar Z, et al. Rupture spontanée de l’utérus non cicatriciel pendant le travail: À propos d’un cas et revue de la littérature: Gynecol Obstet Fertil. 2009; 37: 342.
- Rezapour M, Backstrom T, Ulmsten U. Myometrial steroid concentration and oxytocin receptor density in parturientwomenatterm. Steroids. 1996; 61: 338-344.
- Lim AC, Kwee A, Bruinse HW. Pregnancy after uterine rupture: A report of five cases and a review of the literature. Obstet Gynecol Surv. 2005; 60: 613-617.
- Walsh CA, Reardon W, Foley ME. Unexplained prelabor uterine rupture in a term primigravida. Obstet Gynecol. 2007; 109: 455.