
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Alterations in neutrophil to lymphocyte ratio: An inexpensive, reproducible prognostic marker in patients with complicated liver cirrhosis
Maria Lagadinou*; Charalambos A Gogos; Gerasimos Karantzogiannis; Elena E Solomou
Department of Internal medicine, Patras University Hospital, Rion, Greece.
*Corresponding Author: Maria Lagadinou
Department of Internal medicine, Patras University
Hospital, Rion, Greece.
Email: m_lagad2004@yahoo.gr
Received : Dec 09, 2021
Accepted : Jan 28, 2022
Published : Feb 04, 2022
Archived : www.jcimcr.org
Copyright : © Lagadinou M (2022).
Abstract
Introduction: Liver cirrhosis is generally known as an endstage process where healthy normal liver tissue is replaced by connective tissue. Neutrophil to lymphocyte ratio (NLR) is an inexpensive, readily available and reproducible test and has emerged as a marker of systemic inflammatory response.
Aim: Our study aimed to evaluate the prognostic utility of increased NLR (>3) for patients with liver cirrhosis admitted to hospital due to infection, variceal bleeding or any other cause.
Patients and methods: A total of one hundred twenty cirrhotic patients, who were admitted to the hospital for reasons other than bleeding or sepsis, due to an underlying infection or because of variceal bleeding, were included in the study. Demographic data and laboratory findings were obtained from the patients’ medical record registry and NLR was calculated as the ratio of neutrophils to lymphocytes in the complete blood count on the day of admission.
Results: A statistically significant correlation between NLR and patients’ outcome as well as MELD score was reported in the present study.
Conclusions: Herein we show the value of NLR ratio in the prognosis of cirrhotic patients after hospital admission
Keywords: liver cirrhosis; neutrophil to lymphocyte ratio; outcome; MELD score; prognostic factors.
Citation: Lagadinou M, Gogos CA, Karantzogiannis G, Solomou EE. Alterations in neutrophil to lymphocyte ratio: An inexpensive, reproducible prognostic marker in patients with complicated liver cirrhosis. J Clin Images Med Case Rep. 2022; 3(2): 1637.
Introduction
Liver cirrhosis is generally known as an end-stage process where healthy normal liver tissue is replaced by connective tissue [1]. It is the 12th leading cause of death in the USA. Objective and inexpensive scoring are important prognostic tools for liver cirrhosis. Neutrophil to lymphocyte ratio (NLR) is such an inexpensive, readily available and reproducible test and has emerged as a marker of systemic inflammatory response [2]. Increased number of neutrophils are associated with chronic inflammation while decreased levels of lymphocyte counts are linked with bacterial infection.
It has been shown that increased NLR (NLR>3) is associated with poor clinical outcomes in cardiac diseases and several malignancies [2]. NLR has also been widely used as a prognostic marker for the assessment of patients with various cancers, including gastric cancer, colorectal cancer, breast cancer, lung cancer, ovarian cancer, pancreatic cancer and hepatocellular carcinoma (HCC) [3].
Our study aimed to evaluate the prognostic utility of increased NLR (>3) for patients with liver cirrhosis admitted to the hospital due to an infection, variceal bleeding or any other cause. We wanted to explore any correlation of NLR with parameters related to the cirrhosis stage such as: prothrombin time and the international normalized ratio (INR), albumin and model for end-stage liver disease (MELD) score as well as any potential correlation with the cause of admission and final outcome of cirrhotic patients admitted to the hospital.
Patients and methods
This is a retrospective study carried out at the University Hospital of Patras. The study was approved by the Ethics Committee of the University Hospital of Patras, and written informed consent was obtained from all study subjects included in the study. The diagnosis of cirrhosis was confirmed in all patients with liver biopsy.
A total of one hundred twenty cirrhotic patients, who were admitted to the hospital were included in the study. Patients were stratified in three groups. Patients who were admitted to hospital for reasons other than bleeding or sepsis (i.e. weakness, worsening of ascites, anemia, neurologic complications, dyspnea, chest or abdominal pain, elevated liver enzymes, and jaundice) were included in Group 1 (n= 80), cirrhotic patients admitted due to an underlying infection (pneumonia, spontaneous bacterial peritonitis, urinary tract infection, gastrointestinal tract infection, and soft tissue infection) represented the Group 2 (n=21) and finally in Group 3 all cirrhotic patients with variceal bleeding were included (n=19).
All demographic data were obtained from the patients’ medical record registry (personal history, blood transfusions, alcohol abuse, history of viral hepatitis infection) and laboratory findings (complete blood count, liver function tests, electrolytes, glucose levels, lipid profile, albumin, globulin, neutrophil, lymphocytes counts and PT and APTT tests). NLR was calculated as the ratio of neutrophils to lymphocytes in the complete blood count on the day of admission.
Statistical analysis
Statistical analysis was performed using Statistical Package for the Social Science (SPSS) version 25.0 and significant results were noted as p-value <0.05 obtained from the analysis, Kruskal-Wallis test for statistical analysis was used to determine any significance since the data were not normally distributed. Correlations between NLR were evaluated using Spearman correlation test.
Results
One hundred twenty liver cirrhosis patients, including 103 (85.8%) males and 17 (14.2%) females, were enrolled in the present study. The mean age of the participants was 60.1 ± 12.6 years. The main cause of liver cirrhosis in the study population was alcohol abuse (76.4%). The Group 1 represented the 66.7% of the patients; these patients were admitted to the hospital due to any reason except infection or variceal bleeding. 17.5% of the patients were admitted due to any type of infection (Group 2) while 15.8% due to variceal bleeding (Group 3). Baseline characteristics of patients are presented in Table 1.
Table 1: Clinical characteristics of patients with liver cirrhosis who participated in the study.
Variable |
Total Cohort (n=122) |
Age (year) |
60.1±12.6 |
Male/female, n (%) |
84.4 /15.6 |
Cause of cirrhosis, n(%)
|
76.4 |
MELD score |
18±7.1 |
Cause of admission (%)
NLR according cause of admission
|
15.8 17.5
1.29±0.45 1.24± 0.41 |
NLR (Day 0) according outcome
|
1.22±0.41 |
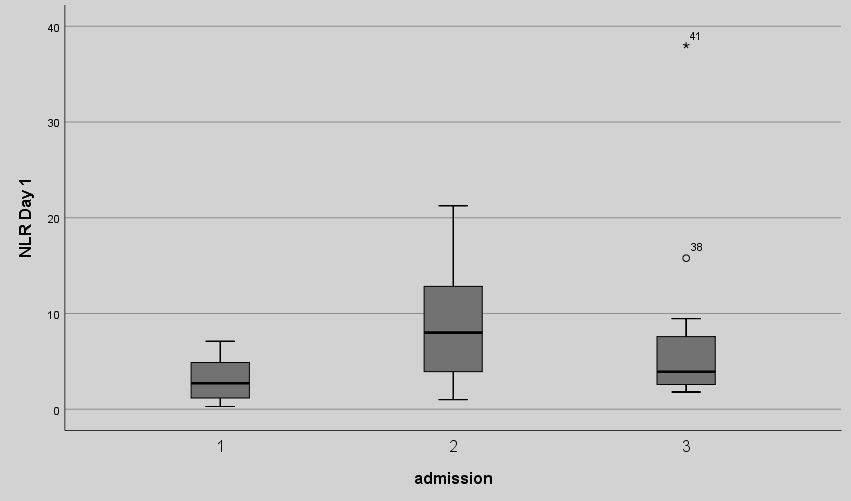
We first examined the NLR ratio on Day 0 (day of admission), between the three groups of patients. We found statistically significant differences between the group of patients who were admitted due to any reason (Group 1) and those who were admitted because of infection (Group 2) (3.18 ± 2.2 vs 9,21 ± 6.3, p:0.002). There was no statistically significant difference of the NLR on Day 0 between Group 1 (patients admitted due to any reason) and Group 3 (variceal bleeding) (3.18 ± 2.2 vs 7.17 ± 0.69, p:0.104) as well as between group 2 and group 3 (9,21 ± 6.3 vs 7.17 ± 0.69, p:0.098). The NLR values are shown in Figure 1a.
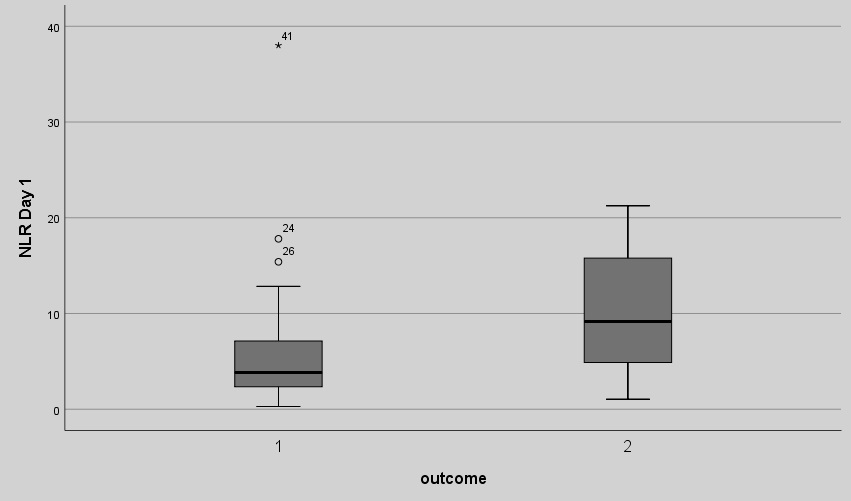
We then examined patients’ outcome based on NLR. A statistical significant correlation between NLR on Day 0 and patients’ outcome (discharge or death during hospitalization) was demonstrated in this study (all patients were included in the analysis). Patients who died had higher NLR ratio compared to those who were discharged (10.21 ± 7.5 vs 5.96 ± 4.8, p: 0.029). The NLR measurements among cirrhotic patients who were discharged and those who died during hospitalization are shown in Figure 1b.
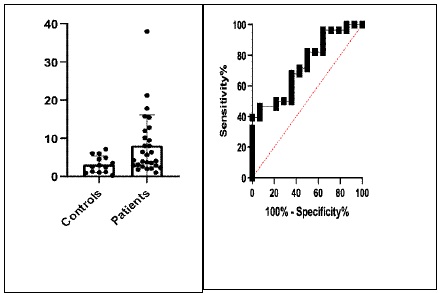
Next, we wanted to explore if there was any difference within groups and categorized patients into high (NLR>3) or low (NLR<3) NLR ratio [1]. Biyik et al found that the mortality rate was significantly higher in patients with an NLR higher than 2.72 compared with lower NLR values. For this reason we also used the NLR cut off value 3. We also performed ROC analysis (Figure 2) and the results showed that the area under curve is 0.702 (95% confidence interval 0.591 to 0.814, p=0.001). We studied the outcome of patients depending on the NLR measurement (>3 or <3) in each group of cirrhotic patients separately and we did not find statistically significant differences in any group: in the group of patients admitted due to any cause other than infection or bleeding p value was 0.587, in the group of patients with any type of infection p value was measured 0.579. Finally, in the group of patients with variceal bleeding p value was measured 0.598. Independently of the group of patients (group 1, group 2 or group 3) we didn’t found statistically significant differences in the final outcome during hospitalization regarding NLR measurement (>3 or <3, p:0.78) too.
Among laboratory tests: complete blood count, liver enzymes, electrolytes (sodium, potassium), creatinine, albumin, globulin, neutrophil, lymphocytes counts, platelets, PT, aPTT and INR tests were studied. NLR was calculated as the ratio of neutrophils to lymphocytes in the complete blood count on the day of admission. Variables including INR and MELD score were statistically significant correlated with higher levels of NLR ratio on admission (day 0) (p: 0.034 and p: 0.031, retrospectively) independently of the cause of admission (infection, variceal bleeding or other). Further analysis, revealed no statistically significant correlation between higher levels of NLR on Day 0 and serum albumin as well as between higher NLR and platelets counts upon admission, in all groups of cirrhotic patients (p:0.168 and p:0.702, retrospectively).
Discussion
NLR is the ratio of neutrophil and lymphocyte counts, and its levels are associated with certain conditions including autoimmune and other diseases. Nevertheless, its applicability on daily clinical basis is useful and very easy to perform in daily practice by clinicians [1].
NLR is an emerging parameter that reflects systemic inflammation, as well as the general nutrition status of patients. It has been reported that malnutrition or hypoalbuminemia correlates well with immune suppression, systemic inflammation and suppression of cell mediated immunity. Systemic inflammation may underlie these conditions. Thus, it has been already reported the relationship between the NLR and nutritional status or immune function [4].
NLR has been shown to predict survival and prognosis in various patient populations with cardiac, malignant and neulogical diseases. Tamhane et al. showed that the NLR value on admission was an independent predictor of in-hospital and 6-month mortality in 2833 patients admitted with a diagnosis of acute coronary syndrome [5]. Furthermore, Switonska et al reported that higher NLR at admission associated with a greater risk of hemorrhagic transformation and neurologicalworsening within the first 24 h from revascularization with intravenous thrombolysis and/or mechanical thrombectomy [6]. Lattanzi et al found higher NLR upon admission were independently associated to poor outcome at 30 days after the intra cerebral hemorrhage onset [7].
The results of our study showed that increased NLR could predict mortality in patients with liver cirrhosis. Generally, there is currently no universal cut-off point for NLR. Interesingly, Biyik et al found that the mortality rate was significantly higher (odds ratio was 8.9) in patients with an NLR higher than 2.72 compared with lower NLR values. [1]. For this reason we also used the NLR cut off value 3 to perform our analysis.
Twelve papers explored the ability of NLR in predicting outcomes of cirrhotic patients. The outcomes contained mortality and infection. Biyik et al. conducted a retrospective observational cohort study to evaluate the role of NLR in predicting long-term mortality in cirrhotic patients without infection. The value of NLR was significantly lower in surviving patients than non-surviving patients [8]. In addition, Kwon JH et al proved that high NLR was associated with one-month survival after admission [1,9].
Patients with cirrhosis have an increased risk of developing bacterial infections due to bacterial overgrowth and increased bacterial translocation. Bacterial infections are a major problem for patients with liver cirrhosis. Elevated NLR has been widely used as a significant predictor factor in patients with liver failure and bacterial infections. Generally, it was proved that elevated levels of NLR are seen in early phase of sepsis and is associated with poor outcome [10].
Although, it has been reported that in uncomplicated cirrhosis, higher NLR could predict mortality independently of the model for end-stage liver disease (MELD) [11], our study reported statistically significant correlation between NLR and MELD score. That is of great importance, since the MELD score was recently introduced to evaluate hepatic function reserve in cirrhotic patients and was also used for survival prediction in cirrhotic patients receiving a transjugular intrahepatic portosystemic shunt. It has also been used to determine priority on waiting lists for liver transplantation and in predicting postoperative outcome of cirrhotic patients, undergoing surgical procedures [12].
Although this is a retrospective, single center study with limited number of patients, our results show that further evaluation of the NLR in cirrhotic patients in a multi-center study setting would be useful.
In conclusion, this is the first study in Greece to explore the value of NLR in the prognosis of cirrhotic patients after hospital admission. Furthermore, the findings of this study will enable further studies of NLR as a surrogate marker for predicting mortality in patients with cirrhosis [13].
Declarations
Declarations of interest: None
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Conflicts of interest/Competing interests: Authors declare no conflict of interest
Contribution: ML: collected and did the analysis of the data and wrote the article, GK: collected the data, GC and EE: critical revision and final approval.
References
- Sun T, Fakhrur RM, Dairi LB, Zain L H. Neutrophil-to-Lymphocyte Ratio (NLR) and its Correlation with Severity of Decompensated Liver Cirrhosis based on Child-Turcotte Pugh (CTP) Score. Journal of Clinical and Diagnostic Research. 2019; 13(2): OC29-OC31.
- Biyika M, Ucarb R, Solakc Y, et al. Blood neutrophil-to-lymphocyte ratio independently predicts survival in patients with liver cirrhosis. European Journal of Gastroenterology & Hepatology. 2013; 25(4).
- Huszno J and Kolosza Z. Prognostic value of the neutrophil lymphocyte, platelet lymphocyte and monocyte lymphocyte ratio in breast cancer patients. Oncology Letters. 2019; 18:6275-6283.
- Sato Y, Gonda K, Harada M et al. Increased neutrophil-to-lymphocyte ratio is a novel marker for nutrition, inflammation and chemotherapy outcome in patients with locally advanced and metastatic esophageal squamous cell carcinoma. BIOMEDICAL REPORTS. 2017; 7:79-84.
- Tamhane U, Aneja S, Montgomery D, Rogers E-K, Eagle A Kim, Gurm Hitinder S. Association Between Admission Neutrophil to Lymphocyte Ratio and Outcomes in Patients With Acute Coronary Syndrome. Am J Cardiol. 2008; 102(6):653-7.
- Switonska M., Pieku´s-Słomka N., Słomka A., Sokal P., Zekanowska E. and Lattanzi S. Neutrophil-to-Lymphocyte Ratio and Symptomatic Hemorrhagic Transformation in Ischemic Stroke Patients Undergoing Revascularization. Brain Sci. 2020; 10:771.
- Lattanzi S, Cagnetti C, Rinaldi C, Angelocola S, Provinciali L. Silvestrini M. Neutrophil-to-lymphocyte ratio improves outcome prediction of acute intracerebral hemorrhage. Journal of the Neurological Sciences. 2018; 387: 98-102.
- Peng Y, Li Y, He Y, et al. The role of neutrophil to lymphocyte ratio for the assessment of liver fibrosis and cirrhosis: a systematic review, Expert review of Gastroenterology and Hepatology, Biomarkers 2018; 12(5):503-513.
- Kwon Hyuk-Chan, Kim Sung Hyun, Oh Sung Yong, et al. Clinical Significance of Preoperative Neutrophil-Lymphocyte Versus Platelet-Lymphocyte Ratio in Patients With Operable Colorectal Cancer. Biomarkers. 2012; 17(3):216-22.
- Kaushik Rajnish, Gupta Monika, Sharma Madhu, et al. Diagnostic and Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Early and Late Phase of Sepsis, Indian J Crit Care Med. 2018; 22(9):660-663.
- Moreau N, Wittebole X, Fleury Y, et al. Neutrophil to lymphocyte ratio predicts death in acute on chronic liver failure patients admitted to the intensive care unit: a retrospective cohort study. SHOCK. 2018; 49(4):385-392.
- Delis SG, Bakoyiannis A, Biliatis I, Athanassiou K, Tassopoulos N & Dervenis C. Model for end-stage liver disease (MELD) score, as a prognostic factor for post-operative morbidity and mortality in cirrhotic patients, undergoing hepatectomy for hepatocellular carcinoma. HPB. 2009; 11:351-357.
- Tanoglua A and Karagoz E. Neutrophil-to-lymphocyte ratio: an emerging prognostic factor of cirrhosis? European Journal of Gastroenterology & Hepatology 2014; 26(3).