
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Neurological injury after transforaminal epidural steroid injection: Rare complication or natural progressive neurological deficit?
Van Boxem K1,2*; Vervoort R1; Hendrix L1; Daenekindt T3; Mesotten D1,3; Van Zundert J1,2
1 Department of Anesthesiology, Intensive Care Medicine, Emergency Medicine and Multidisciplinary Pain Center, Ziekenhuis OostLimburg, Genk, Belgium.
2 Department of Anesthesiology and Pain Management, University Medical Centre Maastricht, Maastricht, The Netherlands.
3 Department of Neurosurgery, Ziekenhuis Oost-Limburg, Genk, Belgium
4 Hasselt University, Faculty of Medicine and Life Sciences and Limburg Clinical Research Center, Diepenbeek, Belgium.
*Corresponding Author: Koen Van Boxem
Department of Anesthesiology, Intensive Care
Medicine, Emergency Medicine, and Multidisciplinary
Pain Center, Ziekenhuis Oost-Limburg, Bessemerstraat,
Lanaken, Belgium.
Email: koen.vb@telenet.be
Received : Nov 06, 2021
Accepted : Feb 01, 2022
Published : Feb 08, 2022
Archived : www.jcimcr.org
Copyright : © Van Boxem K (2022).
Abstract
Transforaminal epidural corticosteroid injections (TFESI) are widely used for subacute lumbosacral radicular pain and are typically applied during the time frame of potential evolution to neurological complications. We present a case report of a patient with lumbar spinal canal stenosis who developed a cauda equina syndrome (CES) after lumbar TFESI requiring emergency decompression. Lumbosacral radicular pain usually has a positive evolution. Some pitfalls may mask progressive neurological deterioration and obscure the causal relation with an epidural corticosteroid injection. An intake consultation with the patient’s informed consent and information on red flags before the procedure is required. If neurological deterioration occurs after a lumbar TFESI, it is sometimes impossible to discriminate the added effect of TFESI to the ongoing progression of neurological deficit. In patients with spinal canal stenosis, the injected volume should preferentially be small to minimize a possible increase in epidural pressure.
Keywords: transforaminal epidural corticosteroid injection; lumbosacral radicular pain; cauda equina syndrome; neurological deficit; spinal canal stenosis.
Abbreviations: CES: Cauda equina syndrome; CT: Computed tomography; EMG: Electromyography; LSS: Lumbar spinal stenosis; MPA: Methylprednisolone acetate; MRC: Medical research council; MRI: Magnetic resonance imaging; TFESI: Transforaminal epidural steroid injection; VP: Vacuum phenomenon.
Citation: Van Boxem K, Vervoort R, Hendrix L, Daenekindt T, Mesotten D, et al. Neurological injury after transforaminal epidural steroid injection: Rare complication or natural progressive neurological deficit?. J Clin Images Med Case Rep. 2022; 3(2): 1642.
Background
Intervertebral disc herniation, lumbar spinal stenosis (LSS), or degenerative vertebrae changes can cause lumbosacral radicular pain [1]. In patients over the age of 65years a progressive segmental degeneration is common [2]. Disc degeneration leads to loss of segmental height, resulting in disc protrusion and spinal canal narrowing. Advanced arthrosis of the facet joints with reactive hypertrophy of the joint and the ligamenta flava additionally narrow the spinal canal and the lateral recesses, causing entrapment and compression of the vascular and nervous structures [3-5]. Older patients with unilateral radicular pain often have a combination of central and neuroforaminal spinal canal stenosis visible on imaging. As stenosis progresses, cauda equina syndrome may develop. It is, however, rare [6]. Transforaminal epidural steroid injections (TFESIs) can be considered in the subacute phase of radicular pain to allow faster healing until spontaneous recovery, thus avoiding surgery in some cases. Although there is no proof of the superiority of surgery or nonsurgical treatment, there are fewer complications with the TFESI [7]. In rare cases often of subacute radicular pain, TFESI can have major neurologic complications [8,9]. In the subacute phase of radicular pain, when TFESIs are used, a progressive neurological deficit is possible, even leading to a cauda equine syndrome.
Case presentation
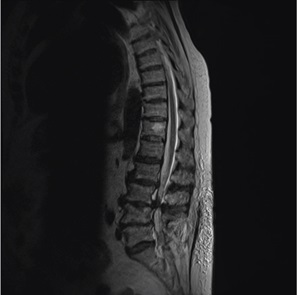
A female patient over 80-year-old, with a history of a laminectomy at level L4-L5, presented at the emergency department with acute L5-S1 radiculopathy and progressive neurogenic claudication, dominant in the right leg, evolving over the last four weeks. Medical conservative treatment in the form of non-steroidal anti-inflammatory drugs could not relieve the pain. In her further history, hypertension and cardiac insufficiency are noted. Vascular clinical examination was normal, and neurological evaluation showed no signs of lower extremity weakness or numbness. There were no signs of cauda equina syndrome (CES). A lumbar magnetic resonance imaging (MRI) showed at L3-4 moderate to severe central spinal canal stenosis, at L4-5 a grade 1 anterolisthesis, at L5-S1 a bilateral limited foraminal narrowing with bilateral extraforaminal disc protrusion with probable bilateral friction with L5 nerve roots (Figure 1). Electromyography (EMG) showed a right radiculopathy L5-S1 without signs of denervation. The patient was admitted to the hospital because of the severity of the pain. The diagnosis of radicular pain was established because of the clear dermatomal distribution, neurogenic claudication, which correlated with EMG and MRI imaging.
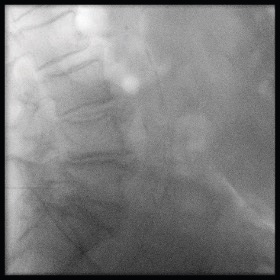
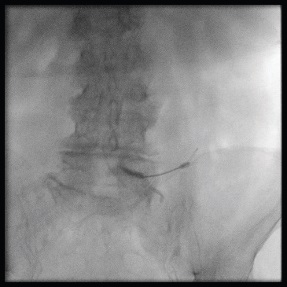
The day after the hospitalization, we performed a right TFESI at the L5 level under fluoroscopic guidance. No sedation was used during the entire procedure. We used the safe triangle approach while maintaining the needle tip posterior in the neuroforamen to avoid the spinal medullary artery (Figure 2 and 3). After injecting contrast under real-time imaging to prevent an accidental intravascular injection, a total volume of 3 ml of 40 mg lidocaine and 40 mg of methylprednisolone acetate (MPA) was injected. During the injection, the patient felt pain, and the injection rate was immediately decreased. The patient returned to the ward without further problems.
The day after the procedure, the nurses of the ward noticed a weakness in the right leg. A clinical assessment showed a paresis of the right foot, both in plantar flexion and dorsiflexion, scaled 2/5 according to the Medical Research Council (MRC) scale, that manually measures the muscle strength. The patient also had diminished anal sphincter tonus and urinary loss, suggestive for a CES. An urgent MRI could not be performed because the patient was unable to lay still for a more extended period due to lumbar pain and pain in the right leg. An urgent Computer Tomography (CT) showed additionally at L4-5 a descending gas containing disc extrusion para-centrally on the right side in contact with an L5 nerve root, which was not visible four days earlier on MRI (Figure 4 and 5). Because of the severity of the symptoms, an emergent laminectomy at levels L2 to L5 was performed. Per-operatively there were no signs of a hematoma or abscess. A repeat EMG 2 weeks after surgery showed significant denervation of the L5 myotome of the right leg. At discharge, one month after the surgery, there was a slight recovery of the motor function, but the patient still needed full walking support. A lower leg orthosis that lifts the foot while walking was custom-made to enhance the patients’ functionality. The pain was significantly reduced three months later, and the patient could walk again with the leg orthosis and a rollator.


Discussion
In this case, a progressive neurological deficit was probably provoked by a new herniated disc but only occurring after the injection since the neurological examination at the emergency department was normal and a new herniated disc not visible on the first MRI 4 days earlier occurred. Therefore, the TFESI given to this patient obscured the causal relation with the new neurological deficit that became more obvious the day after the intervention. Previously reported major neurological complications after epidural corticosteroids include direct needle trauma to the nerve or spinal cord, epidural hematoma and ischemia, infection, the neurotoxic effect of the injected corticosteroid, and accidental intravascular injection of particulate corticosteroids, creating an embolus causing infarction of the conus medullaris at the lumbar level [8].
Wibowo reported a case of CES after caudal epidural sacral injection to treat severe radiating pain in both legs due to lumbar spinal stenosis [10]. Although the authors claim that caudal injections are safer than epidural injections, they found two potential causes for the occurrence of CES: a mechanical problem causing neurological damage and the increased epidural pressure due to the high volume of injected fluid (up to 20ml). These authors report four other cases of neurological deficit after epidural steroid injection in patients with spinal stenosis [11,12].
The contribution of disc herniation to the occurrence of CES was illustrated in a case report where the TFESI was given without previous imaging because the patient could not change into a supine position due to severe pain. The neurological examination showed motor weakness. The patient had no urinary incontinence or saddle anesthesia, and an anal sphincter tone was retained. After the TFESI, the pain was significantly reduced, and the patient underwent an MRI. The patient reported acute paraplegia and complete loss of motor and sensory functions in both legs during the MRI, including sensation around the anus [13]. The MRI showed that the patient’s conus medullaris was above the L1 body and the disc herniation at L1-L2 caused the CES. This case report illustrates the window of time during which symptoms progress. Also, in our case, the contribution of the TFESI to the isolated L5 lesion combined with the CES was initially unclear.
Iatrogenic?
Theoretically, direct needle trauma may worsen the L5 lesion. However, this is unlikely because we positioned the needle correctly using the safe triangle approach. It is also plausible that an acute increase in mass effect attributed to the volume of injectate resulted in ischemia by exacerbating the underlying neuroforaminal stenosis. Despite using fluoroscopy with contrast application, an intravascular injection cannot be entirely ruled out. But this would then more likely give a spinal cord injury with paraplegia rather than a single nerve root injury. However, if the pathophysiology were essentially iatrogenic, this likely would have resulted in acute pain during and after the procedure. This is very unlikely since the patient was transferred to the ward after the procedure without any additional pain.
Natural progression of a herniated disc/cauda equina?
The most probable cause of the nerve injury in combination with the CES seems to be the natural evolution of radiculopathy. The patient was initially hospitalized with progressive neurogenic claudication. No gas-containing disc extrusion was noted on the first MRI but only became apparent at the urgent CT scan after the transforaminal procedure four days after the initial MRI, when the neurological symptoms deteriorated. So, the new disc extrusion probably critically compromised the L5 nerve root and the epidural space on an underlying moderate to severe central spinal canal stenosis L3-4 and anterolisthesis L4- 5, leading to a CES. The estimated incidence of CES is up to 1.9 per 100.000 inhabitants [14]. This contrasts with the prevalence of neurological complications after epidural corticosteroid injections, which can even not be estimated because of the very low incidence [15].The recently published study on serious adverse events after epidural corticosteroid injections in the Medicare population shows an incidence of 8.8 in 1,000,000 patients after lumbar epidural injection. None of these patients had received a transforaminal injection [16]. CES occurs, therefore, more frequently than a neurological complication secondary to an epidural corticosteroid infiltration.
Contributing factors to cauda equine syndrome
In our case, the new herniated disc contained gas, described in the literature as the vacuum phenomenon (VP). Spinal VP within intervertebral disks has a high prevalence in the elderly (>60 years age). It was shown to be exacerbated by extension of the spine and to resolve with flexion. Spinal VP can evolve into disc rupture and sciatica. Moreover spread of gas through ruptured annulus fibrosis allows gas to expand into the epidural space and impinge upon surrounding structures [17]. Gas containing disc extrusions have been described in the literature in patients with acute radiculopathy or exacerbation of chronic pain [18-22]. One case report describes an acute cauda equina syndrome due to a gas-containing prolapsed herniated disc requiring urgent surgery [23].
Further, patients with sciatica and a CES due to a lumbar herniated disc have a significantly smaller epidural space than sciatica patients without CES [24]. Since 1–10% of patients with a known lumbar herniated disc develop CES [24], the chances that an interventional procedure is performed during the timeframe of this natural neurological progression is realistic, thereby obscuring the causal relation with the epidural corticosteroid injection. In patients with spinal stenosis, injection of a small volume is recommended to minimize a possible pressure increase in the epidural space.
Conclusion
Epidural corticosteroid injections are recommended for the treatment of (sub)acute lumbosacral radicular pain. Careful monitoring of the patient during and after the injection is mandatory.
References
- Patel EA, Perloff MD. Radicular Pain Syndromes: Cervical, Lumbar, and Spinal Stenosis. Semin Neurol. 2018; 38(6): 634-9.
- Backstrom KM, Whitman JM, Flynn TW. Lumbar spinal stenosisdiagnosis and management of the aging spine. Man Ther. 2011; 16(4): 308-17.
- Kalff R, Ewald C, Waschke A, Gobisch L, Hopf C. Degenerative lumbar spinal stenosis in older people: current treatment options. Dtsch Arztebl Int. 2013; 110(37): 613-23.
- Manchikanti L, Kaye AD, Manchikanti K, Boswell M, Pampati V, Hirsch J. Efficacy of epidural injections in the treatment of lumbar central spinal stenosis: a systematic review. Anesth Pain Med. 2015; 5(1): e23139.
- Haig AJ, Tomkins CC. Diagnosis and management of lumbar spinal stenosis. JAMA. 2010; 303(1): 71-2.
- Storm PB, Chou D, Tamargo RJ. Lumbar spinal stenosis, cauda equina syndrome, and multiple lumbosacral radiculopathies. Phys Med Rehabil Clin N Am. 2002; 13(3): 713-33.
- Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical Versus Nonsurgical Treatment for Lumbar Spinal Stenosis. Spine (Phila Pa 1976). 2016; 41(14): E857-E68.
- Van Boxem K, Rijsdijk M, Hans G, de Jong J, Kallewaard JW, Vissers K, et al. Safe Use of Epidural Corticosteroid Injections: Recommendations of the WIP Benelux Work Group. Pain Pract. 2019; 19(1): 61-92.
- Ghaly RF, Zouki T, Pynadath A, Candido KD, Knezevic NN. Transforaminal epidural steroid injection can result in further neurological injury in a patient with severe foraminal stenosis and nerve impingement. Surg Neurol Int. 2018; 9: 159.
- Wibowo HA, Rhatomy S. Cauda equina syndrome after caudal epidural sacral injection in severe lumbar spinal stenosis: Case report. Int J Surg Case Rep. 2020; 77: 12-4.
- Seo YT, Kong HH, Lee GJ, Bang HJ. Persistent cauda equina syndrome after caudal epidural injection under severe spinal stenosis: a case report. J Pain Res. 2017; 10: 1425-9.
- Kim D, Kim H. Cauda equina syndrome following epidural adhesiolysis in a patient with spinal stenosis. J Korean Continence Society. 2003; (7): 46-9.
- Jeon SH, Jang W, Kim SH, Cho YH, Lee HS, Ko HC. Paraplegia after transforaminal epidural steroid injection in a patient with severe lumbar disc herniation - A case report. Anesth Pain Med (Seoul). 2021; 16(1): 96-102.
- Woodfield J, Hoeritzauer I, Jamjoom AAB, Pronin S, Srikandarajah N, Poon M, et al. Understanding cauda equina syndrome: protocol for a UK multicentre prospective observational cohort study. BMJ Open. 2018; 8(12): e025230.
- Racoosin JA, Seymour SM, Cascio L, Gill R. Serious Neurologic Events after Epidural Glucocorticoid Injection - The FDA’s Risk Assessment. N Engl J Med. 2015.
- Eworuke E, Crisafi L, Liao J, Akhtar S, Van Clief M, Racoosin JA, et al. Risk of serious spinal adverse events associated with epidural corticosteroid injections in the Medicare population. Reg Anesth Pain Med. 2020.
- Gohil I, Vilensky JA, Weber EC. Vacuum phenomenon: Clinical relevance. Clin Anat. 2014; 27(3): 455-62.
- Choi KC, Kim JS, Lee SH. Surgical experience of gas-containing disk herniation. Neurol Med Chir (Tokyo). 2010; 50(10): 905-9.
- Ryu KS, Rathi NK, Shin MH, Park CK. Gas-containing disc herniations: dual nerve root compression at a single disc level. Neurol Med Chir (Tokyo). 2012; 52(9): 649-51.
- Lee CH, Cho JH, Hyun SJ, Yoon SH, Kim KJ, Kim HJ. Symptomatic gas-containing herniated disc with the vacuum phenomenon: mechanism and treatment. Case report. Neurol Med Chir (Tokyo). 2012; 52(2): 106-8.
- Qasho R, Santoro A, Vangelista T, Cantore G. Nerve root compression by a gas-containing cyst associated with stenotic lateral recess. Case report and review of the literature. Journal of neurosurgical sciences. 2001; 45(3): 181-4.
- Kawaguchi S, Yamashita T, Ida K, Ikeda T, Ohwada O. Gas-filled intradural cyst of the lumbar spine. Case report. J Neurosurg. 2001; 95(2 Suppl): 257-9.
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012; 380(9859): 2224-60.
- Korse NS, Kruit MC, Peul WC, Vleggeert-Lankamp CLA. Lumbar spinal canal MRI diameter is smaller in herniated disc cauda equina syndrome patients. PLoS One. 2017; 12(10): e0186148.