
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Testis sparing surgery in small testicular masses: A case report of adenomatoid tumor
Sofia Giannone1*; Gabriele Tulone1; Rosa Giaimo1; Marco Vella1; Davide Baiamonte1; Piero Mannone1; Nicola Pavan2; Alchiede Simonato1
1 Department of Surgical, Oncological and Oral Sciences, Section of Urology, University of Palermo, Palermo, Italy
2 Urology Clinic, Department of Medical, Surgical and Health science, University of Trieste, Trieste, Italy.
*Corresponding Author: Sofia Giannone
Department of Surgical, Oncological and Oral
Sciences, Section of Urology, University of Palermo,
Palermo, Italy
Email: Sofia.giannone@gmail.com
Received : Jan 03, 2022
Accepted : Feb 01, 2022
Published : Feb 08, 2022
Archived : www.jcimcr.org
Copyright : © Giannone S (2022).
Abstract
The testis sparing surgery is a safe and feasible procedure for patients with small testicular masses, which are defined in literature as not palpable and/or <2 cm in diameter masses, and may be benign in 80% of cases. We report our experience on TSS of one patient with small testicular nodules, that was diagnosed as an adenomatoid tumor.
Keywords: testis sparing surgery, small testicular masses, adenomatoid tumor, testicle tumor.
Citation: Giannone S, Tulone G, Giaimo R, Vella M, Baiamonte D, et al. Testis sparing surgery in small testicular masses: A case report of adenomatoid tumor. J Clin Images Med Case Rep. 2022; 3(2): 1643.
Introduction
The testis sparing surgery (TSS) was proposed in 1986 thanks to Stoll [1], and due to the increasing use of imaging exams (US, MRI and CT) and frozen section examination (FSE), the technique is became more common in the field of surgery for incidental small masses and more safe for the patients. The TSS is particularly useful in the small testicular masses (STM), which are defined in literature as not palpable and/or <2 cm in diameter masses, and may be benign in 80% of cases [2].
We report our experience on TSS of one patient with small testicular nodules, that was diagnosed as an adenomatoid tumor thanks to the frozen section examination. The surgical technique used differs slightly from the technique described by Goldstein, and it is described in the following article [2] (Figure 1).
Case presentation
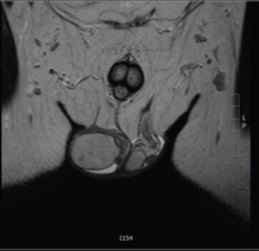
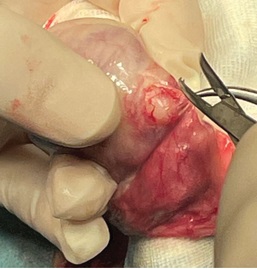
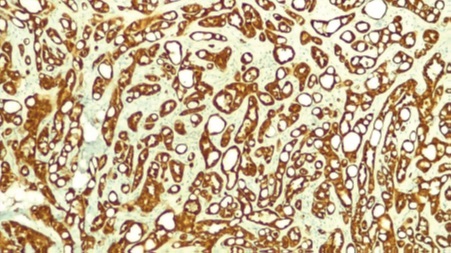
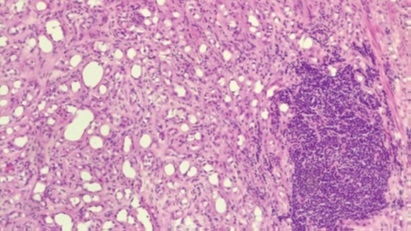
A 54 year-old patient complained pain and a palpable small mass in the right testis. There were no other genitourinary symptoms and the past medical history was negative for other pathologies. At the clinical examination a 1 cm round, painful, not tender mass was confirmed on the right side in the tail of epididymis. Bilateral hydrocele was revealed, scrotal skin, spermatic cords, and the other testis were completely normal. During the examination an ultrasonography of the testis was performed. US showed the hypoechoic small mass (1 X 1 cm) in the tail of the epididymis. The laboratory investigations were performed and testicular tumor markers beta –HCG, alfa-feto protein and LDH were within the normal limit. An MRI was also achieved. The imaging showed an oval mass in contiguity to the tail of right epididymis with a maximum diameter of about 0.8 cm, hypo-isointense with the didymus in T2 sequences (Figure 2), not endowed with signal restriction in DWI and endowed with marked post-contrast enhancement, with absence of lymphadenomegaly. A suspected diagnosis of adenomatoid tumor was supposed at the MRI. After informed consent, a scrotal exploration and a testis sparing surgery was performed. During the surgery at the lower pole of the right didymus a solid formation of about 1 cm was documented (Figure 3). The frozen section examination was negative for neoplastic tissue, so the procedure was concluded. The complete histopathological examination showed a nodular mass formed by proliferation of elements medium-sized epitheliomorphs organized in tubular structures and without significant cytoatipies. Immunohistochemical exams showed Calretinin + (Figure 4), PanCK+ (Figure 5), D2-40+, CK5/6+, Ki67: 2%, OCT4. Such morphological and immunophenotypic findings were consistent with adenomatoid tumor.

Discussion
Testis-sparing surgery may be performed for benign <2 cm lesions such as adenomatoid tumor, teratoma, Leydig cell tumor, and epidermoid cyst based on imaging characteristics and frozen biopsy findings [1]. The TSS should be mandatory performed together with frozen section examination because cancer can be present even in very small masses (<1 cm) or in not palpable masses, so if a cancer is detected an orchidectomy will be the right therapeutic choice. In benign masses the TSS avoids unnecessary radical intervention, so from reduce psychosocial consequences related to a modified body-image, and save endocrinal function to avoid hypogonadism and infertility [3]. A meticulous clinical and instrumental evaluation, with US or MRI, allow an accurate selection of patient eligible for organ-preserving surgery. After a literature revision, we have collected a total of 20 cases of Adenomatoid tumor treated with TSS. Table 1 summaries some notable characteristics of patients undergoing this type of surgery. As the table shows, TSS is a technique performed in different areas of the world, and can be easily and safetly performed in case of negative tumor markers and after an imaging stadiation (US or MRI). Aspiration cytology was reported only in two patients.
Table 1: A literature revision about Adenomatoid tumor treated with TSS. Summary of some notable characteristics of patients undergoing this type of surgery.
study |
years |
country |
Number of patients |
Age/ |
pain |
Synchronous/ |
Tumor size |
Tumour markers |
Diagnostic tools |
R.Gonzalez Resina et al.[4] |
200-2008 |
Spain |
9 |
49.6 |
NA |
no |
NA |
negative |
NA |
Yozo Mitsui et al.[5] |
2008 |
Japan |
1 |
44 |
no |
no |
13mm |
negative |
Ultrasonography, MRI |
Manisha Makkar et al.[6] |
2013 |
India |
1 |
41 |
yes |
no |
25mm |
negative |
Ultrasonography Aspiration citology, |
Duqun Chen et al.[7] |
2006-2013 |
China |
2 |
39.5 |
no |
no |
15mm |
negative |
Ultrasonography |
Sonu Gupta et al.[8] |
2012 |
India |
1 |
24 |
no |
no |
15mm |
negative |
Ultrasonography Aspiration citology of the swelling |
YE Jian-Fei et al.[9] |
2019 |
China |
3 |
42.6 |
NA |
no |
10mm |
negative |
Ultrasonography |
Murat keske et al.[10] |
2008-2017 |
Turkey |
2 |
NA |
NA |
One patient |
20mm |
negative |
NA |
Andrea B.Galosi et al.[11] |
2016 |
Italy |
1 |
60 |
NA |
no |
8.8mm |
negative |
NA |
In our case, patient has a common presentation of adenomatoid tumor from the tail of the epididymis associated with scrotal pain. The clinical examination, negative markers and imaging investigations were probative for a diagnosis of adenomatoid tumor. Although clinical and radiological investigations are able to distinguish some benign lesions, to be certain of the best treatment a Testis-sparing surgery with frozen section examination must be planned, so as to confirm the benign origin of the mass during the surgical procedure; although clinical and radiological investigations are able to distinguish some benign lesions.
References
- Campbell, Walsh, Wein. Urology - Twelfth Edition. Elsevier. 2020; 76: 1709.
- De Stefani S, Isgrò G, Varca V, Pecchi A, Bianchi G, Carmigliani G. et al. Microsurgical Testis-sparing surgery in small testicular masses: seven years retrospective managmente and results. Urology. 2012; 79(4): 858-62.
- Benelli A, Varca V, Derchi L, Gregoli A, Carmigliani G, Simonato A. Evaluation of the decision – making process in the conservative approach to small testicular masses. Urologia. 2017; 84(2): 83-87.
- González Resina R, Carranza Carranza A, Congregado Córdoba J, Conde Sánchez JM, Congregado Ruiz CB, Medina Lopez R. et al. Paratesticular adenomatoid tumor: a report of nine cases. Actas Urol Esp. 2010; 34(1): 95-100.
- Mitsui Y, Ueda Y, Suzuki T, Shincho M, Higuchi Y, Qui J. et al. A case of adenomatoid tumor of the testis treated by testis-sparing surgery: a case report. Hinyokika Kiyo. 2008; 54(5): 383-6.
- Makkar M, Dayal P, Gupta C, Mahajan NC. Adenomatoid tumor of testis: A rare cytological diagnosis. Journal of Cytology. 2013; 30(1): 65-67.
- Chen D, Yu Z, Ni L, Gui Y, Yang S, Shi B. et al. Adenomatoid tumors of the testis: A report of two cases and review of the literature. Oncology letters. 2014; 7(5): 1718-1720.
- Gupta S, Garg S, Agarwal R, Sen R. Aspiration cytology of adenomatoid tumor of epididymis: An important diagnostic tool. JSCR. 2012; (4): 11.
- Ye JF, Wang B, Ma LL, Zhao L, Wang GL, Hong K. Organ-sparing partial orchietectomy for testicular adenomatoid tumor. Journal of Peking University. Health Sciences. 2019; 51(2): 365-368.
- Keske M, Canda AE, Atmaca AF, Cakici OU. Arslan ME, Testissparing surgery: Experience in 13 patients with oncological and functional outcomes. Can Urol Assoc J. 2019; 13(3): E83–E88.
- Galosi AB, Fulvi P, Fabiani A, Servi L, Filosa A, Leone L. et al. Testicular sparing surgery in small testis masses: A multinstitutional experience. Archivio Italiano di Urologia e Andrologia. 2016; 88(4): 320-324.