
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Imaging of descending necrotizing mediastinitis: A report of 11 cases and review of the literature
Hajar Adil1*; Laila Jroundi2; Fatima Zahrae Laamrani3
Department of Emergency Radiology, University Hospital Ibn Sina, Abderrahim Bouabid Avenue, Rabat, Morocco
*Corresponding Author: Hajar Adil
Department of Emergency Radiology, University
Hospital Ibn Sina, Abderrahim Bouabid Avenue,
Rabat, Morocco.
Email: hajaradil1991hajara@gmail.com
Received : Nov 08, 2021
Accepted : Feb 03, 2022
Published : Feb 10, 2022
Archived : www.jcimcr.org
Copyright : © Adil H (2022).
Abstract
Introduction: Descending necrotizing mediastinitis is a rare and fatal condition that results from the spread of cervicofacial infections to the mediastinum. Early and appropriate management is needed to reduce mortality and morbidity rates. Imaging, especially CT, plays a central role in the diagnosis, treatment, and monitoring of patients. This study is aimed at assessing the role of computed tomography in diagnosing and planning the management of DNM.
Material and methods: This is an 8-year retrospective study on 11 patients who fulfilled the ESTRERA criteria. All the patients underwent thoracic radiography along with an enhanced cervicothoracic CT scan.
Results: Median age was 34 years with a sex-ratio of 1.75. 4 patients had diabetes. The primary oropharyngeal infection was an odontogenic abscess in most cases. The reported symptoms were mainly thoracic pain and fever. Thoracic radiography and cervicothoracic CT scan confirmed the diagnosis and showed different findings. 7 patients were diagnosed with type I DNM, 1 patient with type IIA and 3 patients with type IIB.
Conclusion: DNM is a medico-surgical emergency where imaging, in particular CT, plays an essential role in establishing the diagnosis and guiding the surgical approach to ensure optimal patient care.
Keywords: descending necrotizing mediastinitis; deep neck infection; CT; emergency.
Citation: Adil H, Jroundi L, Laamrani Z. Imaging of descending necrotizing mediastinitis: A report of 11 cases and review of the literature. J Clin Images Med Case Rep. 2022; 3(2): 1648.
Introduction
Descending Necrotizing Mediastinitis (DNM) is a rare but fatal form of acute mediastinitis that occurs when neck infections extend to the mediastinum through deep facial spaces [1]. Early diagnosis and adequate treatment are essential to minimize mortality. Computed Tomography (CT) is an integral part of the management of DNM as it confirms the diagnosis and guides the surgical procedure [2]. The objective of this paper is to assess the role of computed tomography in diagnosing and planning the management of DNM.
Case presentation
The patients included 7 men and 4 women (sex-ratio:1,75). The median age was 34 years (range, 22-70 years). 4 patients had diabetes. The intervals between onset of symptoms and hospitalization varied from 5 to 30 days (mean 15 days). The primary oropharyngeal infection was an odontogenic abscess (n=8, 73%), cervical soft tissue abscess (n=2, 18%), and peritonsillar abscess (n=1, 9%). The reported symptoms were mainly cervicothoracic pain, erythema, tenderness, and fever. 6 patients presented with thoracic pain and dyspnea.
Thoracic radiography showed a widening of the mediastinum in 7 patients, pleural effusion in 4 cases and pulmonary infiltrates in 4 patients.
Enhanced cervicothoracic CT scan was performed on all our patients and confirmed the diagnosis of DNM, showing variable findings as represented in “Table 1”.
Table 1: Cervicothoracic CT findings.
|
Cases |
Mediastinal fat infiltration |
10 |
Mediastinal emphysema |
3 |
Mediastinal fluid collections |
7 |
Pleural effusion |
5 |
Pericardial effusion |
2 |
Mediastinal lymphadenopathy |
9 |
Subcutaneous emphysema |
3 |
Pulmonary infiltrates |
6 |
Pulmonary embolism |
1 |
Osteitis |
2 |
7 patients were diagnosed with type I DNM, 1 patient with type IIA and 3 patients with type IIB.
The patients were initially admitted to the Intensive Care Unit (ICU) where they received broad-spectrum antibiotics together with airway management. All of our patients underwent surgical intervention according to the type of DNM.
The postoperative course was unremarkable for 5 patients, 3 patients required prolonged hospitalization in the ICU, mean while, 3 patients died of septic shock.
Discussion
DNM is an uncommon form of acute mediastinitis that results from the spread of a severe cervico-facial infection to the mediastinum (odontogenic infections, peritonsillar and retropharyngeal abscesses, traumatic pharyngeal perforations) [3,4]. It is a rare and rapidly progressive condition with reported mortality rates ranging from 20 to 40% especially if diagnosis and treatment are delayed [5-7]. DNM predominantly affects young men and people with immunocompromising conditions [8-11]. Early recognition of DNM is critical, before the spread of the infection to the mediastinum and development of sepsis [5]. Signs of a deep cervical infection such as swelling, erythema, and tenderness, are usually present at first. Mediastinal involvement should be suspected whenever dyspnea, dysphagia, and thoracic pain are found [3,4,12,13].
The Estrera’s diagnostic criteria remain valid to establish the diagnosis of DNM [8]:
1- Clinical manifestations of severe infection
2- Demonstration of characteristic radiographic features such as mediastinal widening, mediastinal emphysema, mediastinal fluid collection with bubbles or abscesses with air-fluid level
3- Preoperative or post-mortem documentation of such infection
4- Establishment of a relationship between an ongoing oropharyngeal or cervical infection and the mediastinal necrotizing process.
Medical imaging plays a central role in the diagnosis and management of DNM.
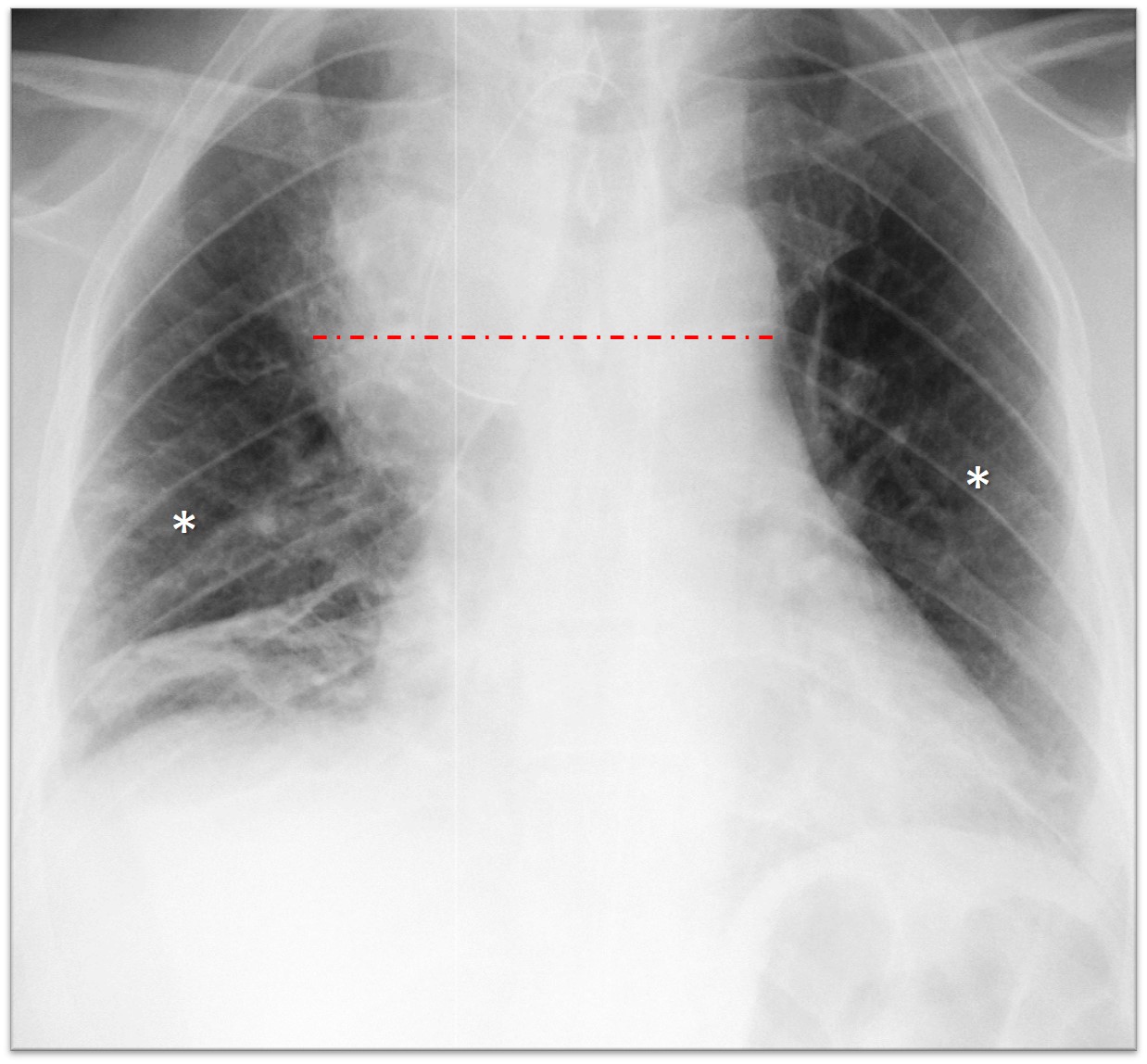
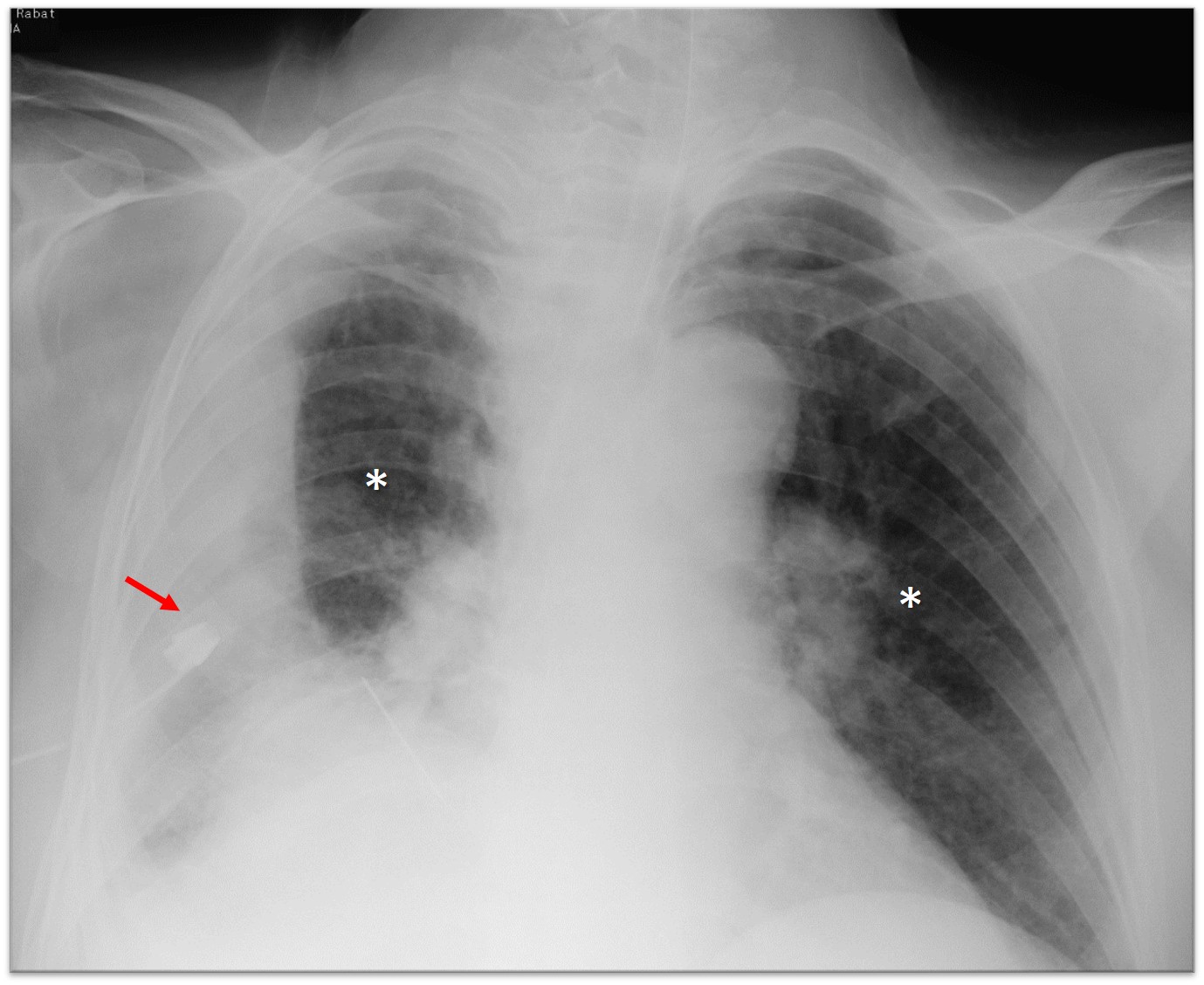
Plain chest radiography is the first line of imaging technique performed on patients with respiratory symptoms. It commonly uses a standard posteroanterior projection. The radiologic findings in plain chest radiography are the following [5,14]:
Mediastinal emphysema - Widening of the mediastinum (Figure 1) - Pleural, pericardial effusion (Figure 2) - Opacity filling the retro-sternal, retro-cardiac spaces - Pulmonary infiltrates (Figures 1,2)
Cervicothoracic CT scan is the modality of choice for DNM imaging as it confirms the diagnosis and gives important information concerning the extent and the severity of mediastinal involvement [14-16].
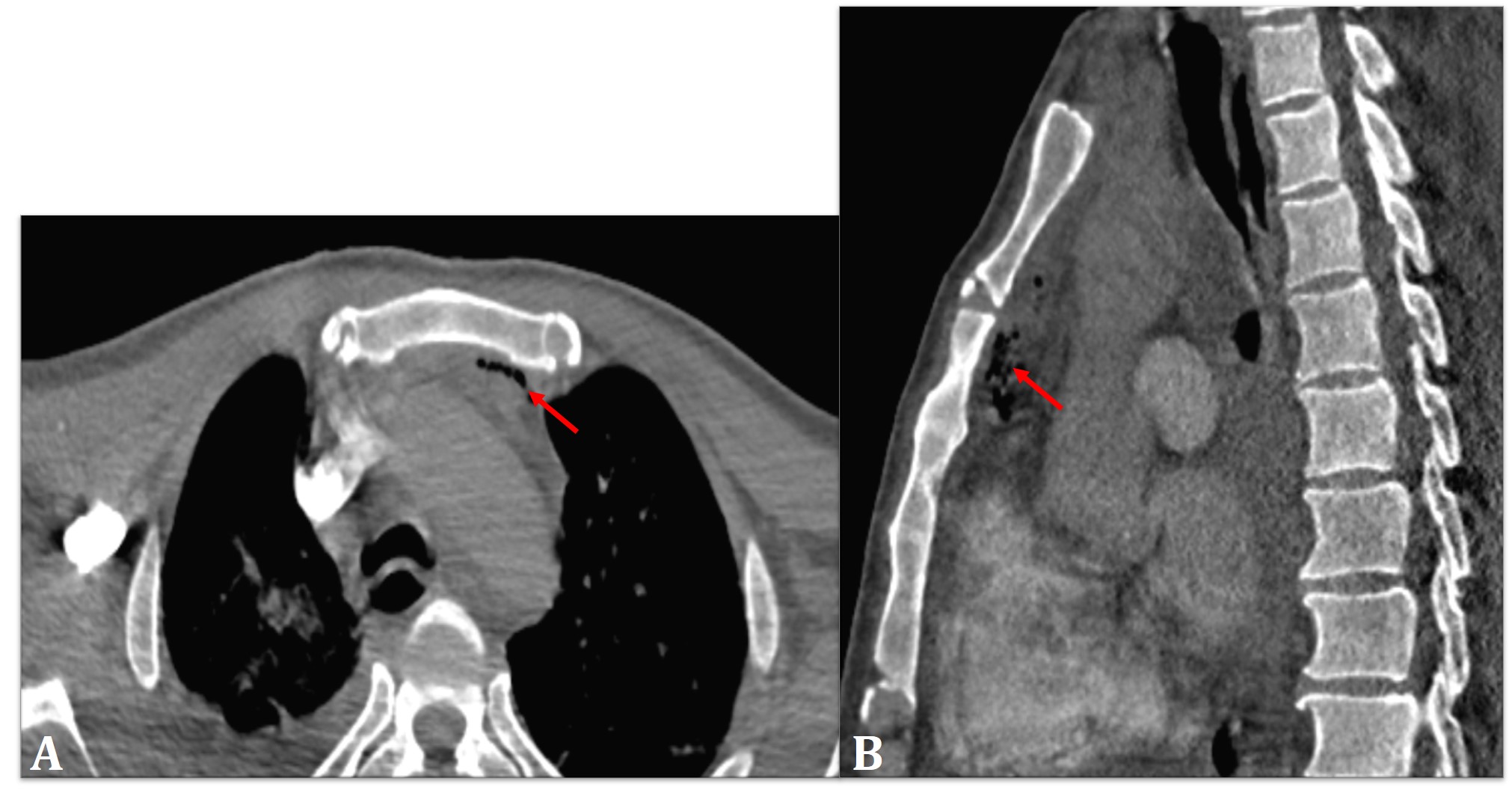
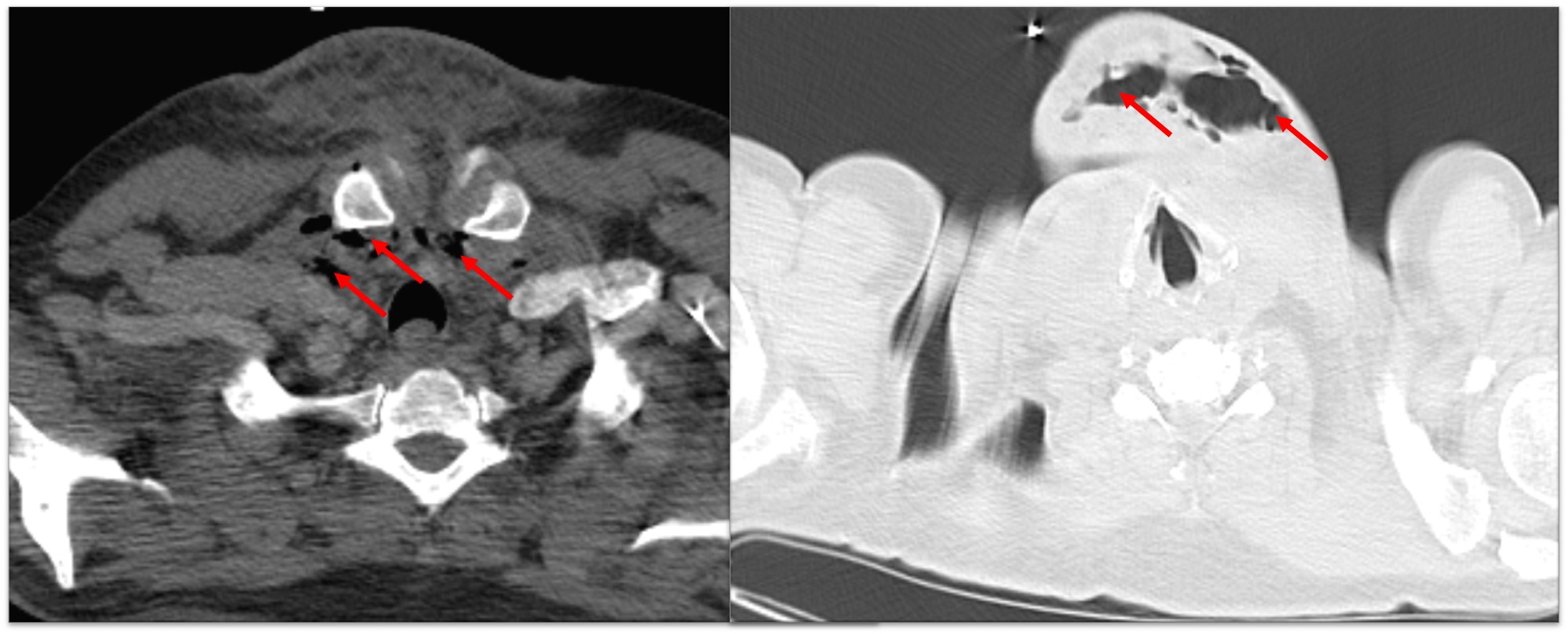
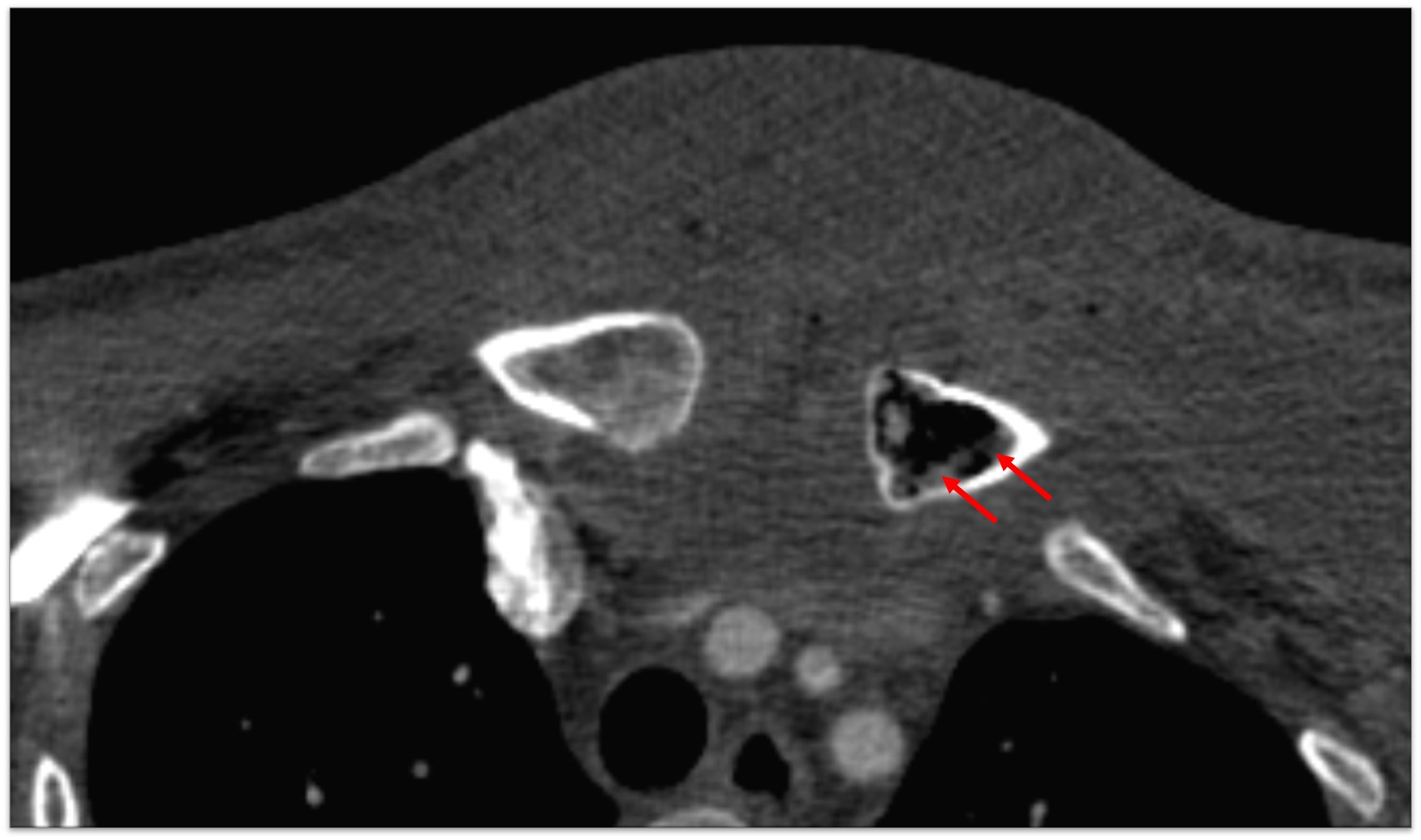
The examination protocol includes two helical acquisitions covering the area from the skull base to the diaphragm before and after a bolus of 2 cc/Kg intravenous contrast media. Image reconstruction is done in thin slices. Studies are transferred to a viewing workstation where multiplanar CT reformatted scans are viewed. The following features of DNM can be identified [2, 5,14]:
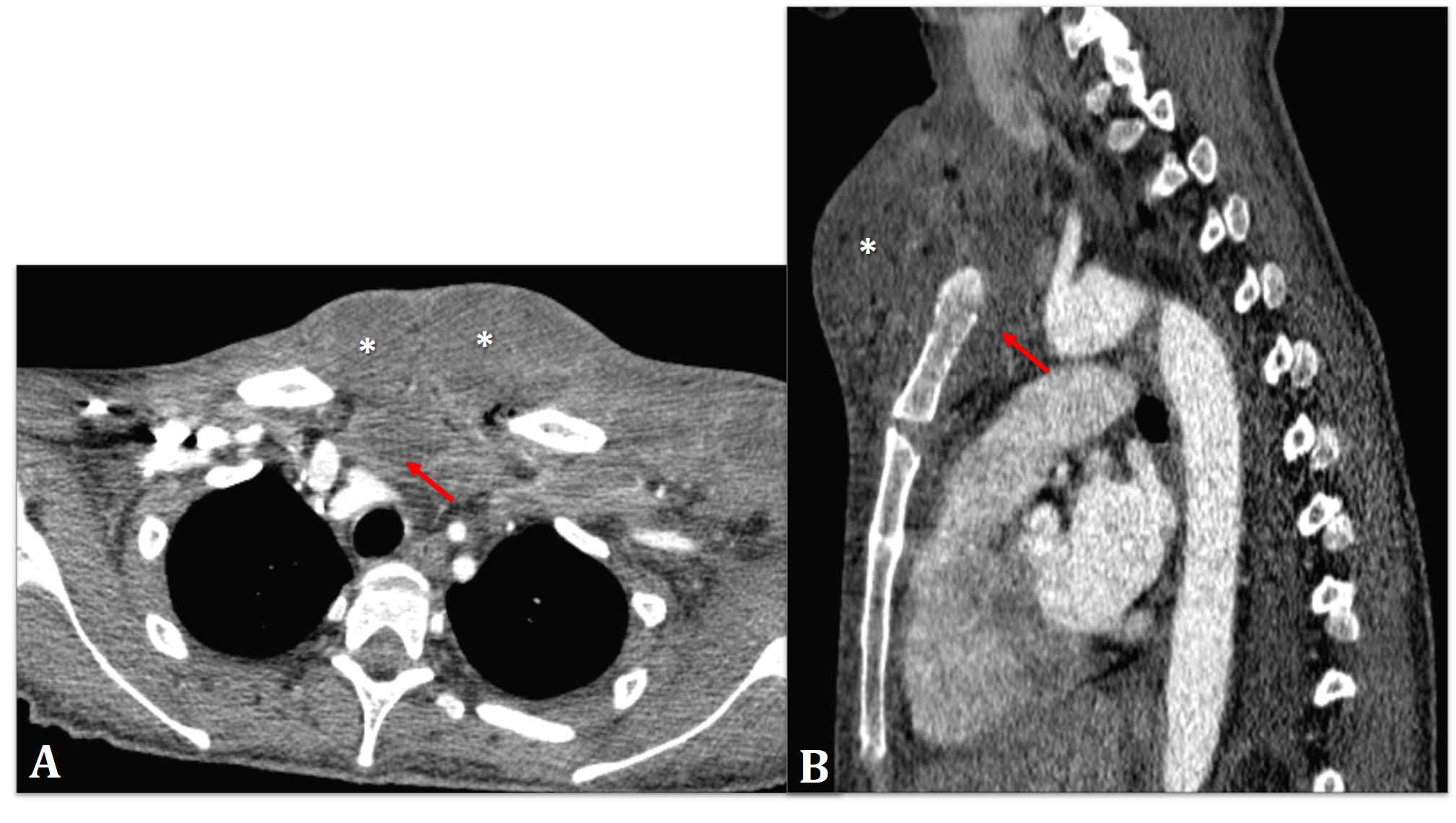
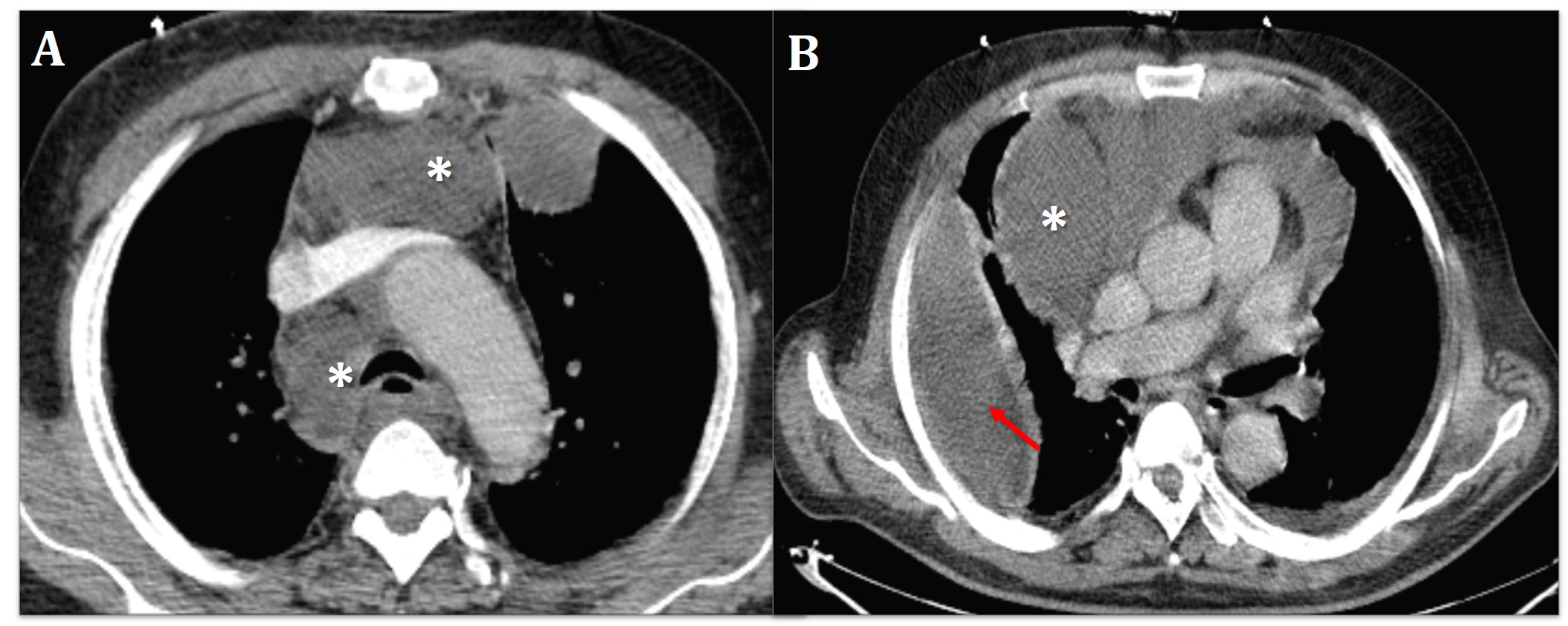
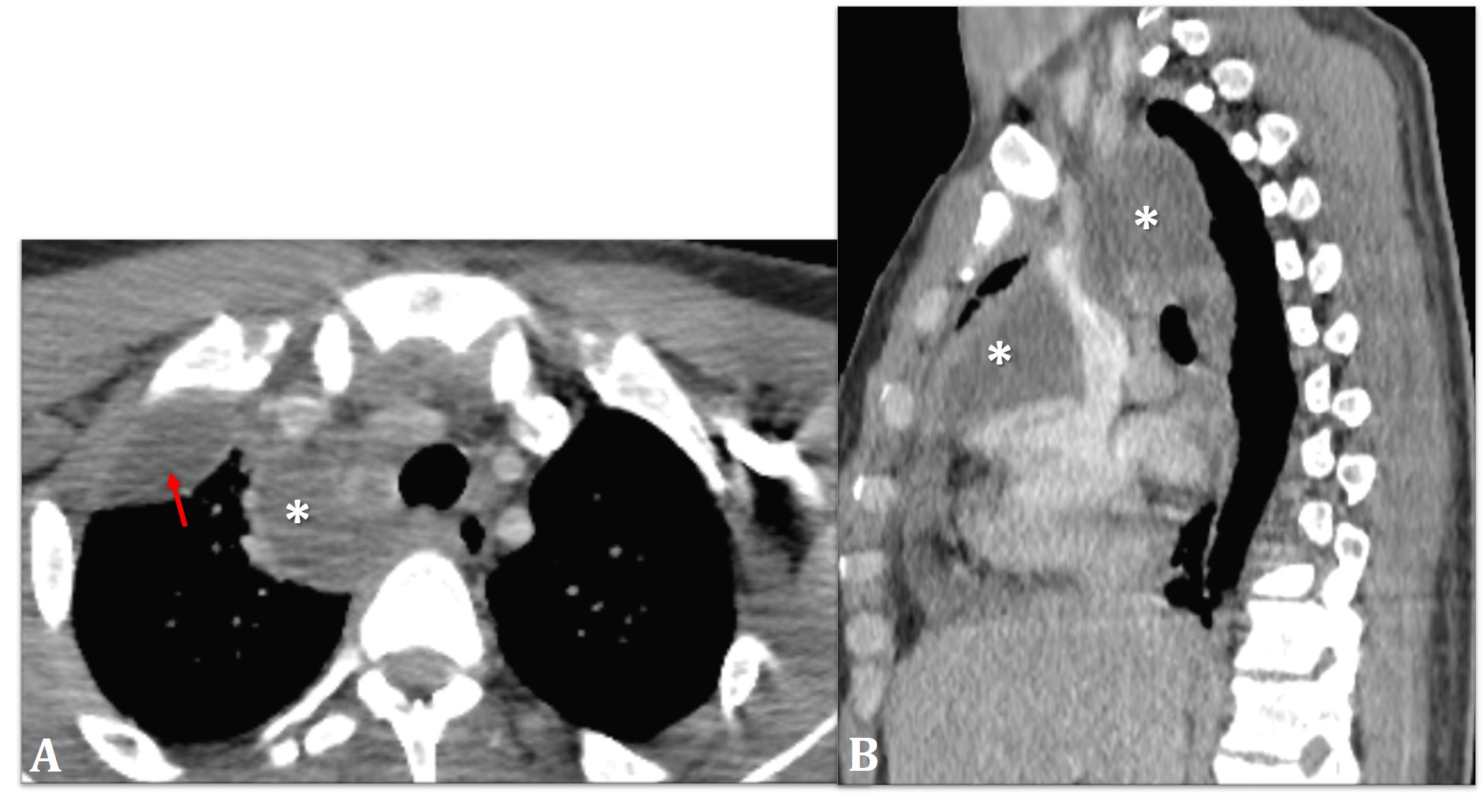
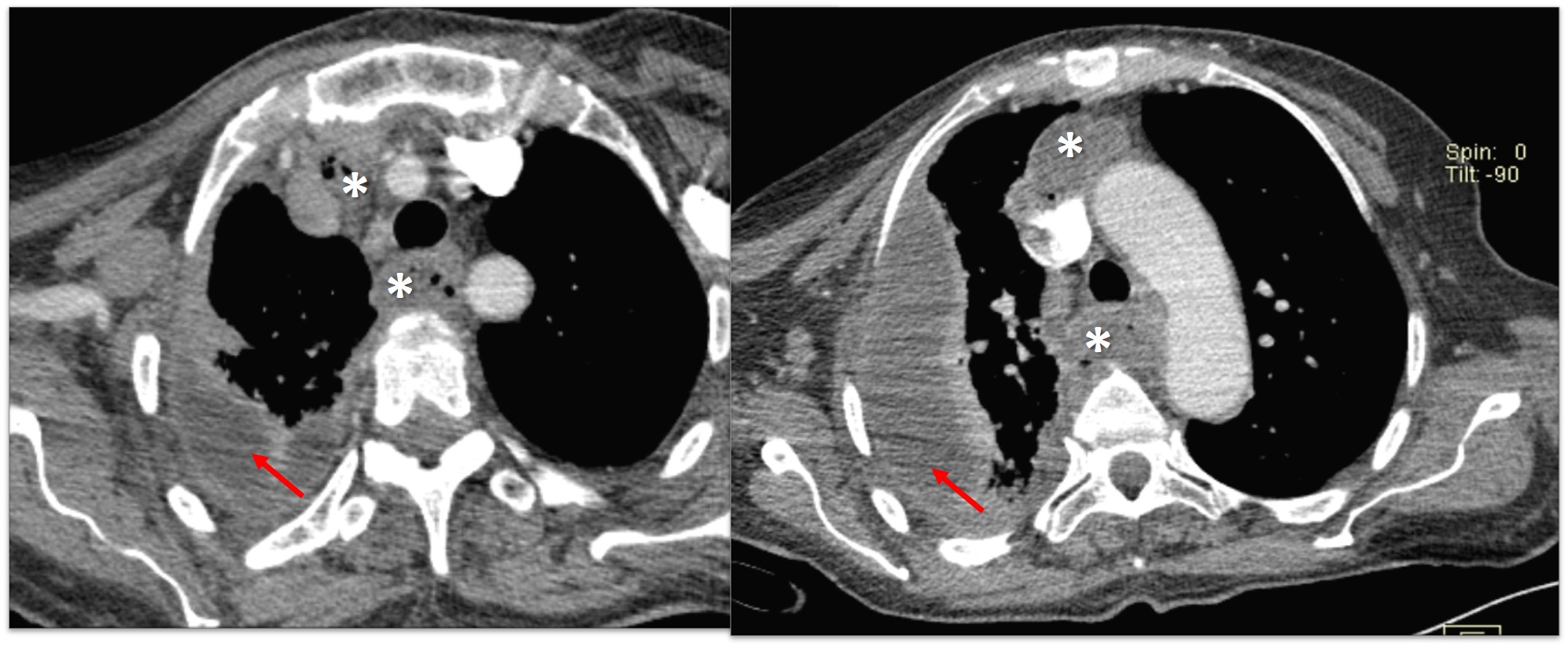
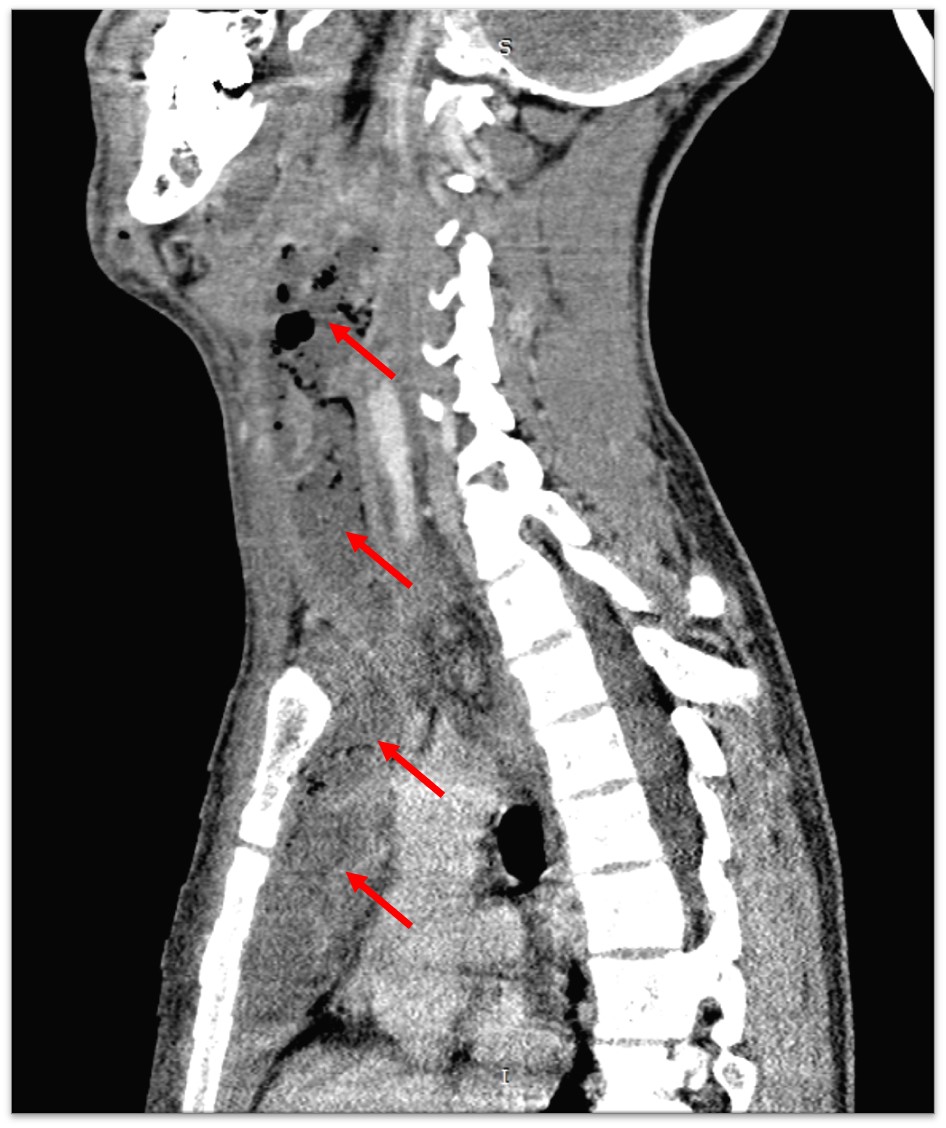
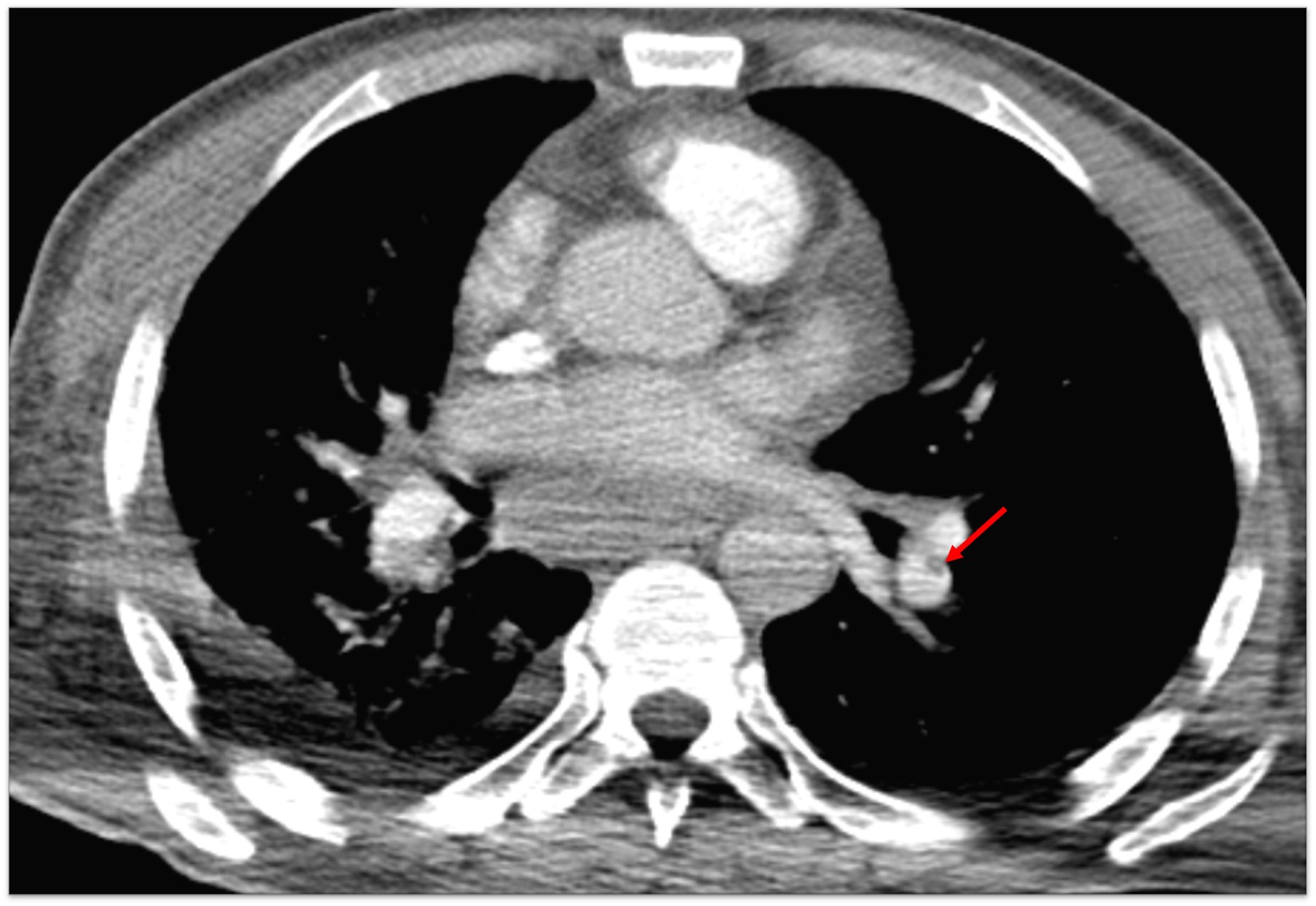
- Mediastinal fat infiltration (increased density) (Figure 3) - Mediastinal emphysema (Figure 3) - Mediastinal fluid collections with or without gas (Figures 4-8) - Pleural, pericardial effusion (Figures 5-7) - Myositis and thickened muscular fascia - Cervical, mediastinal lymphadenopathy - Subcutaneous and soft tissue emphysema (Figure 9) - Osteitis of sternum, clavicle (Figure 10) - Vascular thrombosis (Figure 11)
Hasegawa and Endo classified DNM into three types according to its diffusion within the mediastinum, based on CT findings [2,5,17]:
- Type I: The infection is limited to the upper mediastinum, above the carina - Type IIA: The infection spreads down to the anterior mediastinum - Type IIB: The infection extends under the carina to the anterior and posterior mediastinum.
Hence, the CT scan guides surgical and drainage procedures. It is also a useful tool to monitor the adequacy of mediastinal drainage after surgery and for the decision-making to re-operate if the infection persists or relapses within the mediastinum [2,18].
DNM should be treated adequately and promptly to reduce mortality. Treatment is mainly based on [12,19-22]:
- surgical cervical and mediastinal debridement and drainage. - effective pleural and pericardial drainage - administration of appropriate broad-spectrum antibiotics - airway management and support of the vital organs in the ICU Surgical debridement approach depends on the type of DNM, defined by Hasegawa and Endo classification [5,14]: - type I: Cervicotomy with mediastinal drainage by a cervical approach. - type IIA: Cervicotomy and thoracic drainage through a substernal incision - type II B: Debridement following irrigation of the mediastinum through a standard right thoracotomy, followed by a minimal left thoracotomy.
Conclusion
DNM remains a life-threatening condition that requires rapid diagnosis and treatment. The use of CT scan is critical to help improve clinical outcome, as it diagnoses early-stage DNM and guides surgical approaches. CT can be useful to assess postoperative results to indicate possible reoperation in patients who still show signs of infection.
Declarations
Acknowledgment: This research did not receive any specific subsidy from public, commercial or not-for-profit funding organizations.
Conflict of interests: The authors declare that they have no links of interest.
References
- Pearse HE. Mediastinitis Following Cervical Suppuration. Ann Surg. 1938; 108: 588-611.
- Scaglione M, Pinto A, Giovine S, Di Nuzzo L, Giuliano V, Romano L. CT features of descending necrotizing mediastinitis-a pictorial essay. Emerg Radiol. 2007; 14: 77-81.
- Liptay MJ, Fry WA, Shields TW. Acute and chronic mediastinal infections. General Thoracic Surgery. 5th ed. Philadelphia, PA: Lippincott Williams and Wilkins. 2000; 20: 93-104.
- Yanık F, Karamustafaoğlu YA, Yoruk YJTJoIiDC. Management of a difficult infectional disease: Descending necrotizing mediastinitis. 2018; 12: 748-754.
- Foroulis, Christophoros N, Sileli MN. Descending necrotizing mediastinitis: Review of the literature and controversies in management. The Open Surgery Journal. 2011; 5.
- Ridder Gerd J, Wolfgang Maier, Susanne Kinzer, Teszler CB, Boedeker CC, et al. Descending necrotizing mediastinitis: Contemporary trends in etiology, diagnosis, management, and outcome. Annals of surgery. 2010; 251: 528-534.
- Kocher, Gregor J, Beatrix Hoksch, Marco Caversaccio, Jan Wiegand, et al. Diffuse descending necrotizing mediastinitis: Surgical therapy and outcome in a single-centre series. European journal of cardio-thoracic surgery
- Estrera AS, Landay MJ, Grisham JM, Sinn DP, Platt MR, et al. Descending necrotizing mediastinitis. Surg Gynecol Obstet. 1983; 157: 545-552.
- Wheatley, Michael J, Stirling MC, Kirsh MM, Otto Gago, et al. Orringer. Descending necrotizing mediastinitis: Transcervical drainage is not enough. The Annals of thoracic surgery. 1990; 49: 780-784.
- Mathieu D, Neviere R, Teillon C, Chagnon JL, Lebleu N, Wattel F. Cervical necrotizing fasciitis: Clinical manifestations and management. Clin Infect Dis. 1995; 21: 51-56.
- Iwata I, Takekazu, Yasuo Sekine, Kiyoshi Shibuya, Kazuhiro Yasufuku, et al. Early open thoracotomy and mediastinopleural irrigation for severe descending necrotizing mediastinitis. European journal of cardio-thoracic surgery. 2005; 28: 384-388.
- Marty-Ané, Charles-Henri, Jean-Philippe Berthet, Pierre Alric, Jean-Dominique Pegis, et al. Management of descending necrotizing mediastinitis: An aggressive treatment for an aggressive disease. The Annals of thoracic surgery. 1999; 68: 212-217.
- Corsten MJ, Shamji FM, Odell PF, Frederico JA, Laframboise GG, Reid KR, et al. Optimal treatment of descending necrotising mediastinitis. Thorax. 1997; 52: 702–708.
- Pinto, Antonio, Mariano Scaglione, Maria Giuseppina Scuderi, Giovanni Tortora, et al. Infections of the neck leading to descending necrotizing mediastinitis: Role of multi-detector row computed tomography. European journal of radiology. 2008; 65: 389-394.
- Novellas S, Kechabtia K, Chevallier P, Sedat J, Bruneton JN. Descending necrotizing mediastinitis: A rare pathology to keep in mind. Clinical imaging. 2005; 29: 138-140.
- Anil Kumar B, Chandramohan S, Parasu N. Case of the month. Acute neck swelling. Br J Radiol. 2005; 78: 89-90.
- Endo, Shunsuke, Fumio Murayama, Tsuyoshi Hasegawa, Shinichi Yamamoto, et al. Guideline of surgical management based on diffusion of descending necrotizing mediastinitis. The Japanese Journal of Thoracic and Cardiovascular Surgery. 1999; 47: 14-19.
- Ho, MW, Dhariwal DK, Chandrasekhar J, Patton DW, Silvester KC, et al. Use of interventional radiology in the management of mediastinitis of odontogenic origin. British Journal of Oral and Maxillofacial Surgery. 2006; 44: 538-542.
- Vigne Ph, Duvillard Ch, Romanet Ph. Les cellulites cervicales diffuses. Oto-Rhino-Laryngologia Nova. 1999; 9: 245-251.
- Freeman, Richard K, Eric Vallieres, Verrier ED, Riyad Karmy Jones, et al. Descending necrotizing mediastinitis: An analysis of the effects of serial surgical debridement on patient mortality. The Journal of thoracic and cardiovascular surgery. 2000; 119: 260-267.
- Mitjans MS, Sanchís JB, Padro XB, García I, Garolera JM, et al. Descending necrotizing mediastinitis. Int Surg. 2000; 85: 331- 335.
- Kiernan PD, Hernandez A, Byrne WD, Bloom R, Dicicco B, et al. Descending cervical mediastinitis. Ann Thorac Surg. 1998; 65: 1483-1488.