
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Prevalence, clinical manifestations and co-infections of buruli ulcer in parts of Imo State, Nigeria
Chijioke JV Odaghara1; Bertram EB Nwoke2; Chinyere N Ukaga2; Luke C Nwosu3*
1 Department of Biology/Microbiology, Federal Polytechnic Nekede, Owerri, Nigeria.
2 Department of Animal and Environmental Biology, Imo State University, Nigeria.
3 Department of Crop and Soil Science, University of Port Harcourt, Nigeria.
*Corresponding Author: Luke C Nwosu
Department of Crop and Soil Science, University of
Port Harcourt, Nigeria.
Email: luke2007ambition@yahoo.com
Received : Nov 26, 2021
Accepted : Feb 04, 2022
Published : Feb 11, 2022
Archived : www.jcimcr.org
Copyright : © Nwosu LC (2022).
Abstract
The study investigated prevalence, clinical manifestations and co-infections of buruli ulcer in parts of Imo State, Nigeria. The sampled human population was physically examined for buruli ulcer infection, in ulcerative stages wound swab samples were collected using sterile swab sticks and taken to the laboratory for microbial analysis. Microbial analysis of samples, gram staining, and identification of bacterial isolates, biochemical tests and determination of co-infections were achieved using standard methods. The analysis of results revealed moderately high prevalence rate of buruli ulcer disease in the area. The results further showed that in Oguta 58.54% of sampled individuals had clinical manifestations of the infection. Ohaji/Egbema recorded 51.46 %, Oru East had 57.50% of victims with clinical manifestations, Onuimo had 61.29%, Isiala Mbano recorded 60.00 %, Ikeduru 54.14% and Oru-West had 53.42% of individuals with clinical manifestations of buruli ulcer. Prevalence of the buruli ulcer differed among the Local Government Areas studied. Study revealed variations in prevalence and clinical manifestations between males and females in the communities surveyed, with more females having ulcerative cases, too. Bacterial isolates confirmed from buruli ulcer disease were Staphylococcus aureus, Bacillus spp., Proteus spp., Pseudomonas aeruginosa and Streptococcus spp. Candida albicans, a fungal species was also isolated. Different microbial species responsible for pus formation in buruli ulcer wounds were highlighted. The results revealed that the toxin produced by Staphylococcus aureus caused dermatitis and toxic shock syndrome to the victims.
Keywords: buruli ulcer infection; biochemical test; prevalence rate; bacterial isolates; toxic shock syndrome.
Citation: Odaghara CJV, Nwoke BEB, Ukaga CN, Nwosu LC. Prevalence, clinical manifestations and co-infections of buruli ulcer in parts of Imo State, Nigeria. J Clin Images Med Case Rep. 2022; 3(2): 1652.
Introduction
The actual burden of buruli ulcer disease and number of victims have not been adequately estimated especially in terms of the psycho-social effects on the most neglected population in Nigeria [4,9,13]. The same authors stressed that the number of persons affected annually remains uncertain. In Nigeria, Chukwuekezie et al. (2007) reported twenty-four buruli ulcer cases in and around Ibadan. Pre-assessment sensitization workshops for health workers within the selected Nigerian States were held in June and July 2006 [4]. The team (which was made up of international experts, national and state officials) was divided into two groups for better coverage and awareness on prevalence of buruli ulcer disease. Based on World Health Organization case definition, 14 of 37 patients examined were likely to have buruli ulcer (9 active and 5 inactive cases) and 9 were children less than 15 years of age. Eight patients were females and 6 were males. One of the patients with active disease had the edematous form, one had osteomyelitis and ulcer and the other 7 had ulcers. Ten of the patients had lesions on the lower limbs, three on the upper limbs, and one on the face [2]. These are documented indications of clinical manifestations. In 4 (44%) of the 9 buruli ulcer patients with active cases, the clinical diagnosis was confirmed by the IS2404 PCR at the Institute of Tropical Medicine [4]. Information in literature shows that buruli ulcer still persist in Nigeria and other countries of the world [1,6]. Therefore, absence of regular reports on the prevalence and clinical manifestations of buruli ulcer and co-infection cases in Nigeria further justify the present investigation. From community reports, buruli ulcer cases are rising in Nigeria and may be more prevalent than previously thought particularly in Imo State, Nigeria, where there is clear dwindling environmental sanitation and vulnerable habits among the people. It is against this background that the current study was designed with the specific objectives to determine prevalence, clinical manifestations and co-infections in buruli ulcer in some parts of Imo State, Nigeria.
Materials and Methods
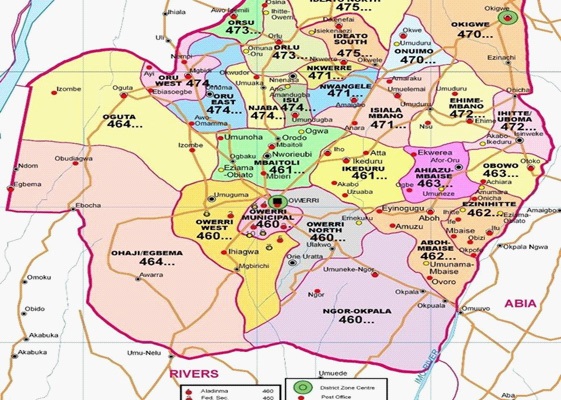
The study area
This study was conducted in some parts of Imo State, Nigeria (Figure 1). Imo State is part of the tropical humid region of Nigeria where climatic factors, environmental conditions and human activities can easily predispose individuals to buruli ulcer infection. Imo State lies between latitude 7’45’ and ‘6 15 North and Longitude 80 and 89 East. The Local Government Areas selected and studied were Ohaji/Egbema, Oguta, Ikeduru, Isiala-Mbano, Oru-East, Onuimo and Oru-West.
Design and sampling
Across-sectional design comprising interviews and focus group discussions was adopted and applied in 2018 and 2019. The systematic sampling technique with 10 % coverage was ensured.
Instrument for data collection, validation and reliability test
Apart from visual and medical observations, well-structured questionnaires were developed to harness complemented information on buruli ulcer prevalence, clinical manifestations and co-infections. The questionnaire was validated in Imo State University, Owerri Nigeria and Alvan Ikoku Federal College of Education, Owerri, Nigeria. After validation, the instrument was tested for reliability using Cronbach’s Alpha Coefficient [7].
Physical examination of sampled population
In the sampled communities, a total of one thousand, two hundred and twenty six individuals were physically examined at the Health Centres for different stages of clinical manifestations of buruli ulcer disease. This ranged from nodule, oedema, and plaque and to ulcerative lesions. The German Leprosy and Tuberculosis Relief Association in co-operation with National Tuberculosis and Leprosy Control Programme provided active help. The study lasted from August 2015 to June 2019. The exercise provided the opportunity to gather relevant information on prevalence too.
Collection of samples
A total of two hundred and twenty six people whose buruli ulcer infection appeared to have reached ulcerative stage, were called for wound swab samples collections using sterile swab sticks and taken to the laboratory for microbial analysis. Positive cases were recorded and expressed in percent for males and females.
Microbiological analysis of samples
The swab samples were placed in nine milliliter (9.0 ml) of nutrient broth contained in a test tube and allowed to stand for about ten minutes to obtain a wash water of the wound swab samples; thereafter one milliliter (1.0 ml) of the wash-water was serially diluted using tenfold serial dilution. After the serial dilution, 0.1 ml of the 10”1 dilution was ascetically inoculated onto sterile plates of Nutrient agar, Mac Conkey agar and Saboraud Dextrose agar standard culture media for enumeration of microorganisms. After inoculating the sterile media, they were incubated at 37°C for 24 hours for the bacteriological media and at 27°C for 48 hours for the mycological media. After the incubation periods, the microorganisms enumerated on the culture plates were counted using the colony counter. The microbial isolates obtained were thereafter identified using culture morphology. The bacterial isolates were further characterised using gram staining and biochemical tests [8,5]. The fungal isolates were further characterised using lactophenol cotton blue staining techniques.
Diagnosis, specimen culture and determination of co-infections
The ulcer exudates and biopsy specimens were cultured and incubated at 32°C for 6-8 weeks incubation period to grow Mycobacterium ulcerans using Ogawa and Lowestein-Jensen culture media. The culture is 20-60% sensitive. Other co-infections infecting the ulcer wounds were also identified by culturing ulcer exudates and biopsy specimens using Mac-Conkey agar, blood agar and chocolate agar media to isolate both aerobic and anaerobic bacteria.
Statistical analysis
Descriptive statistics of frequencies, percentages and counts were used to analyse data and the results were summarized in the result tables.
Results and discussion
Table 1 shows that varying human population in the seven Local Government Areas were positive and had clinical manifestations of buruli ulcer infection. In Oguta, 58.54% of sampled individuals were infected. Ohaji/Egbema recorded 51.46%, Oru East had 57.50% of infected victims, Onuimo had 61.29%, Isiala Mbano recorded 60.00%, Ikeduru 54.14% and Oru-West had 53.42% of individuals with buruli ulcer. There was significant difference (P < 0.05) in the prevalence of the buruli ulcer infections among the Local Government Areas sampled. Table 2 shows gender-related ulcerative stages of buruli ulcer disease in selected parts of Imo State, Nigeria. There were more females (134) than males (92) with ulcerative infected cases. In Oguta there were 44.44% males and 55.56% females with buruli ulcer disease. Clinical manifestation data show that Ohaji\Egbema had 47.22% males and 52.78% females, Oru East had 41.67% males and 58.33% females, Onuimo had 30.95% males and 69.05% females, Isiala Mbano 38.89% males and 61.11% females, Ikeduru Local Government Area recorded 40.63% males and 59.37% females, and in Oru West, 47.06% males and 52.94% females examined had buruli ulcer diseases. Table 3 presents gender-related clinical manifestation of buruli ulcer among the people examined. There were more females (415) than males (279). In Oguta 45.00% males and 55.00% females, Ohaji/Egbema 38.46% males and 61.54% females, Oru East had 43.48% males and 56.52% females, Onuimo 35.96% males and 64.04% females, Isiala Mbano 34.41% males and 65.59% females, Ikeduru 40.00% males and 60.00% females and Oru West 44.19% males and 55.81% females. The results of the morphological characteristics of bacteria isolated from buruli ulcer disease are presented in Table 4. Table 5 shows the fungal isolates. The study revealed moderately high prevalence rate of buruli ulcer disease in the area. The variations in prevalence rate recorded in the different parts of Imo State suggest that buruli ulcer infection is location-specific and this provides the justification for further location-specific studies. The study revealed variations in prevalence and clinical manifestations between males and females in the communities investigated. Higher prevalence in female individuals recorded in this study is an index of peculiarities associated with domestic and commercial activities of women. Co-infection investigations showed that the bacterial isolates obtained from buruli ulcer disease were Staphylococcus aureus, Bacillus spp., Proteus spp., Pseudomonas aeruginosa and Streptococcus spp. The fungal isolate, Candidaalbicans was also obtained. Thus, different microbial species were responsible for the pus formation in buruli ulcer wounds. The most common-pus producing bacteria identified were Staphylococcus aureus, Klebsiella spp. Psuedomonas spp., Escherichia coli and Streptococcus spp. Staphylococcus aureus is a gram positive cocci which is a facultative anaerobe. Suffice it to say that some Staphylococcus aureusspecies are coagulasepositive and having golden yellow colonies. Unfortunately, the toxin produced by Staphylococcus aureus caused dermatitis and toxic shock syndrome. This is supported by literature [10,6]. In literature, Staphylococcus aureus has often been encountered and thought to be acquired infection. However, the problem with Staphylococcus aureus becomes more complicated when it was found that it quickly develops resistance and was capable of producing many antibiotic resistance strains. This is very common in hospitals where drug resistance hospital strains have been reported [3,11,13]. Of the numerous organisms that colonise chronic wounds, wound-care experts believe that Staphylococcus aureus, Pseudomonas aeruginosa, beta-hemolytic Streptococcus and anaerobes are the most likely bacterial causes of delayed healing and infection. The significance of S. aureus (whether a pathogen or a coloniser) in a chronic wound is difficult to ascertain. We found that clinical manifestations of buruli ulcer are easily evident; but the mode of transmission of buruli ulcer remains undoubtedly unclear. A more severe form of infection produces diffuse swelling of a limb, unlike the papule or nodule which can be painful and accompanied by fever. Infection may frequently follow physical trauma [13] and this was confirmed in the present study. Findings further revealed that the severity of buruli ulcer and associated symptoms depended on whether the disease was at the ulcerative stage or not, in most of the communities sampled, and this is consistent with the reports of WHO [12,13]. Protective clothing such as rubber boots, improved hygiene, clean environment, early report and diagnosis, consultation of medical experts instead of quacksand Government being proactive to neglected tropical diseases will reduce prevalence rate, limit co-infections and minimize mortality associated with buruli ulcer disease.
Table 1: Prevalence of buruli ulcer/ clinical manifestations in the selected parts of Imo State, Nigeria .
L.G.A. |
No. |
NHCLM |
% HCLM |
NWOCLM |
%WOCLM |
Oguta |
205 |
120 |
58.54 |
85 |
41.46 |
Ohaji/ |
202 |
104 |
51.46 |
98 |
48.54 |
Oru-East |
160 |
92 |
57.50 |
68 |
42.50 |
Onuimo |
186 |
114 |
61.29 |
72 |
38.71 |
Isiala Mbano |
155 |
93 |
60.00 |
62 |
40.00 |
Ikeduru |
157 |
85 |
54.14 |
72 |
45.86 |
Oru West |
161 |
86 |
53.42 |
75 |
46.58 |
NHCLM: Number that Had Clinical Manifestations; %HCLM: Percentage that Had Clinical Manifestations; NWOCLM: Number Without Clinical Manifestations; %WOCLM: Percentage Without Clinical Manifestations; Note: Percent prevalence/ clinical manifestations were computed per Local Government Area.
Table 2: Gender-related ulcerative stage prevalence of buruli ulcer disease in selected parts of Imo State, Nigeria.
L.G.A. |
Ulcerative |
Male |
Female |
% Male |
% Female |
Oguta |
27 |
15 |
15 |
44.44 |
55.56 |
36 |
36 |
17 |
19 |
47.22 |
52.78 |
Oru-East |
36 |
15 |
21 |
41.67 |
58.33 |
Onuimo |
42 |
13 |
29 |
30.95 |
69.05 |
Isiala Mbano |
36 |
14 |
22 |
38.89 |
61.11 |
Ikeduru |
32 |
13 |
19 |
40.63 |
59.37 |
Oru West |
17 |
8 |
9 |
47.06 |
52.94 |
Table 3: Gender-related buruli ulcer clinical manifestationsin the selected Local Government Areas of Imo State, Nigeria.
L.G.A. |
No. |
NHCLM |
Male |
Female |
%Male |
%Female |
Oguta |
205 |
120 |
54 |
66 |
45.00 |
55.00 |
Ohaji/Egbema |
202 |
104 |
40 |
64 |
38.46 |
61.54 |
Oru-East |
160 |
92 |
40 |
52 |
43.48 |
56.52 |
Onuimo |
186 |
114 |
41 |
73 |
35.96 |
64.04 |
Isiala Mbano |
155 |
93 |
32 |
61 |
34.41 |
65.59 |
Ikeduru |
157 |
85 |
34 |
51 |
40.00 |
60.00 |
Oru West |
161 |
86 |
38 |
48 |
44.19 |
55.81 |
Total |
1226 |
694 |
279 |
415 |
|
|
Table 4: Morphological and biochemical characteristics of bacteria isolates in the study.
Sample media |
Morphological |
Oxidase test |
Motility test |
Indole test |
Spore stain |
Catalase test |
Citrate test |
Possible bacteria |
BCNA |
Milkishmucoid colonies |
Gram positive cocci |
- |
- |
- |
- |
+ |
Staphylococcus aureus |
BCNA |
Pale flat colonies |
Non-gram positive rod |
- |
- |
- |
+ |
- |
Bacillus spp |
BCNA |
Bluish green pigmented |
Gram negative rod |
+ |
+ |
- |
- |
+ |
Pseudomonas aeruginosa |
BCNA |
Milkish non-mucoid colonies growing in chains |
Gram positive cocci |
- |
- |
- |
- |
- |
Non-reaction streptococcus spp |
BCNA |
Pale elongated mucoid colonies spread over the pale |
Gram negative rod |
- |
- |
+ |
+ |
- |
Proteus spp |
KEY: N.A: Nutrient Agar; + : Positive; -: Negative; S: Slope Colouration; B: Butt Colouration; G: Gas Production; H2S: Hydrogen Sulphide Production; Y: Yellowish Colouration (acidic); Reddish Pinkish Colouration (Alkaline Production); Mot: Motility.
Table 5: Identification of fungal isolates in the study.
Sample |
Macroscopic |
Microscopic |
Possible fungi |
BU |
Creamy raised non Mucoid colonies |
Budded yeast cells |
Candida spp |
Conclusion
The findings from this study would make available preliminary information on the epidemiology of buruli ulcer in Imo State, Nigeria. Moderately high prevalence of buruli ulcer disease was recorded. Prevalence and clinical manifestations were higher in females than males and varied among the Local Government Areas. The study revealed some isolates of Mycobacterium ulcerans present in Imo State. Education of the rural communities during the study has enhanced awareness on early detection, diagnosis, treatment and reports which are vital aspects of prevention and control strategies of buruli ulcer. The study has revealed that microorganisms associated with buruli ulcer are Staphylococcus aureus, Streptococcus species, Pseudomonas aeruginosa, Klebsiella species and Candida species. These organisms have been implicated in the delay of woundhealing. The baseline information on buruli ulcer in parts of Imo State, Nigeria could be used to promote evidence-based policies for the control of buruli ulcer in any other part of the world.
References
- Asiedu K, Raviglione M, Scherpbier R. ed. Report, International conference on Buruli ulcer control and Research Yamaissaikro, d’Ivoire 6-8 July 1998. Geneva, World Health Organization, 1998. (document WHO/TB/98.252).
- siedu K, Raviglione M, Scherpbier R eds. Buruli ulcer: Mycobacterium ulcerans infection. (WHO/CDS/CPE/GBUI/2000.1). Geneva: World Health Organization; 2000.
- Barker DJ. Buruli disease in a district of Uganda. Journal of Tropical Medicine and Hygiene. 1971; 74: 260-264.
- Buntine J, Crofts K. eds. Buruli ulcer. Management of Mycobacterium ulcerans disease. A manual for health care providers. (WHO/CDS/CPE/GBUI/2001.3). Geneva: World Health Organization; 2001.
- Cheesbrough M. District Laboratory Practice in Tropical Countries, Part Z, Cambridge University Press, Cambridge, UK. 2005.
- Chukwuekezie O, Ampada E, Sopoh G, Dossoi A, Tiendrebeogo A, et al. Buruli ulcer, Nigeria. Emerging Infectious Diseases. 2007; 13: 782-783.
- Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951; 16: 297-334.
- Fawole MO, Oso BA. Characterization of Bacteria. In Labouratory Manual of Microbiology Spectrum Books Limited, Nigeria. 2004; 22-33.
- Gray HH, Kingma S, Kok SH. Mycobacterial skin ulcers in Nigeria. Transactionsof the Royal Societyof Tropical Medicineand Hygiene. 1967; 61: 712-410. 1016/0035-9203(67)90139-3.
- Porteal F. Epidemiology of mycobacterial diseases. Clinics in Dermatology. 1995; 13: 207-222.
- Van der Werf TS, Van der Graaf WT, Tappero JW, Asiedu K. Mycobacterium ulcerans infection. Lancet. 1999; 354: 1013.
- World Health Orgainisation. Working to Overcome the Global Impact of Neglected Tropical Diseases: First WHO Report on Neglected Tropical Diseases. Geneva, Switzerland: World Health Orgainisation. 2010.
- World Health Organisation. Treatment of Mycobacterium ulcerans Disease (Buruli Ulcer): Guidance for Health Workers. Geneva, Switzerland: World Health Orgainisation. 2012.