
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Rhino-orbital mucormycosis in known case of diabetes mellitus type 2, hypertension and ischemic heart disease in post covid status
Girish Mishra; Yojana Sharma; Hetvi Tanna; Harshil Patel*
Otorhinolaryngology Department, Pramukhswami Medical College, Shree Krishna Hospital, Karamsad, Gujarat, India
*Corresponding Author: Harshil Patel
Pramukhswami Medical College, Shree Krishna
Hospital, Karamsad, Gujarat, India.
Email: patel.harshil0098@gmail.com
Received : Dec 01, 2021
Accepted : Feb 04, 2022
Published : Feb 11, 2022
Archived : www.jcimcr.org
Copyright : © Patel H (2022).
Abstract
Mucormycosis is a rare life-threatening fungal infection caused by group of molds called Mucormycetes. Mucormycosis is particularly dangerous because it spreads quickly throughout the body. Left untreated, the infection can spread to the lungs or the brain and may cause brain infection, paralysis, pneumonia, seizures, death [1]. A 66-year-old female with known comorbidity of Diabetes Mellitus, Hypertension and IHD presented to trauma and emergency care with symptoms of LRTI and was tested positive for the COVID-19. She was treated as per COVID-19 protocols. After 15 days she developed headache and left eye swelling and was diagnosed with Mucormycosis for which surgical debridement of sinuses had to be done. Doctors should identify risk factors and should use steroid judicially to prevent rare life-threatening condition. Unfortunately, despite disfiguring surgical debridement and adjunct antifungal therapy, the overall mortality rate for Mucormycosis remains >50%, and it approaches 100% among patients with disseminated disease or those with persistent neutropenia [2,3].
Keywords: mucormycosis; corticosteroids; immunity; diabetes mellitus; COVID-19.
Citation: Mishra G, Sharma Y, Tanna H, Patel H. Rhino-orbital mucormycosis in known case of diabetes mellitus type 2, hypertension and ischemic heart disease in post covid status. J Clin Images Med Case Rep. 2022; 3(2): 1653.
Case presentation
Mucormycosis is an angio-invasive fungal infection, associated with high morbidity and mortality. It is most commonly seen with immune compromised patient. The most common risk factor in India is diabetes mellitus [4]. Mainstay treatment part of covid-19 is steroids which lowers immunity of patients particularly who are diabetics which become risk factor for developing Mucormycosis after covid-19 disease. The prevalence of Mucormycosis in India is about 80 times the prevalence in developed countries, being approximately 0.14 cases per 1000 population [5].
66-year-old female presented to trauma and emergency care of tertiary care center on 19th May, 2021 with chief complain of fever, anorexia, vomiting and generalized weakness for 5 days. As patient was clinically suspected of COVID-19, High Resolution Computed Tomography (HRCT) Chest and Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) was done on admission to confirm the diagnosis. RT-PCR was positive for COVID-19 and multiple peripherally located, predominately subpleural patchy, discrete and confluent ground glass opacity were seen in both the lungs on HRCT Chest which confirmed the diagnosis of COVID-19. CT severity score was 13/25. The patient was hospitalized for further management. Patient had medical history of hypertension for 20 years and was on regular medication. She also had diabetes mellitus for 8 years and was taking Metformin 500 mg BD. She is also known case of Ischemic Heart Disease (IHD) and Coronary Artery Bypass Graft surgery (CABG) was done 2 years back. On admission the deranged investigations were: HbA1c – 7.8%, D-Dimer – 956 ng/mL, CRP – 71.4 mg/L, Serum Creatinine- 1.35 mg/dL.
Patient was treated in critical care unit for 5 days. She was maintaining oxygen saturation 94% on room air and so supplemental oxygen therapy was not required. She was started on Inj. Dexamethasone 4 mg 2-2-2 for 5 days, Inj. Enoxaparin Subcutaneous 0.4 ml 1-0-1 for 5 days, Favipiravir Tab 400 mg 5-0-4 stat followed by 2-0-2 for 6 days and other supportive drugs as per protocol for covid-19 management. Inj. Remdesivir was not given. As patient stabilized, she was discharged after 6 days.
After 15 days, patient presented again in outpatient department with chief complaint of headache in the last 7-8 days and left side eye swelling for 5 days on 9th June 2021. Headache was generalized and continuous in nature. It was not associated with vomiting, neck stiffness, aura, postural changes. After 2-3 days she noticed swelling over her left eye which was gradually increasing in size and was painful. Patient had taken antihistaminic and pain killer medication but symptoms were not relieved. Symptoms were not associated with fever, breathlessness, nausea, anosmia, cough or weakness.
On physical examination patient was vitally stable with pulse rate 84/min, respiratory rate 15/min, blood pressure 110/80 mmHg. No pallor, edema, cyanosis, clubbing, icterus, lymphadenopathy was noted on general examination. On local examination of nose, congestion was present over nasal septum in left nostril. No nasal discharge was seen. On local examination of left eye, swelling was noted. Uniocular and binocular movements were normal, visual acuity was normal, no abnormality detected in right eye. Based on clinical and physical examination patient was suspected for fungal infection and was advised admission for further management.
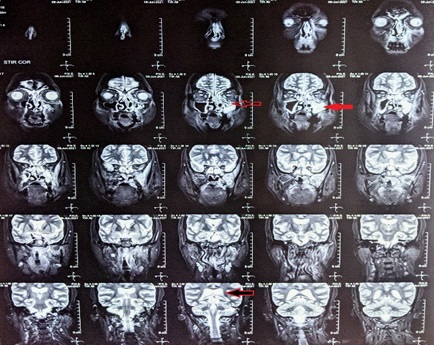
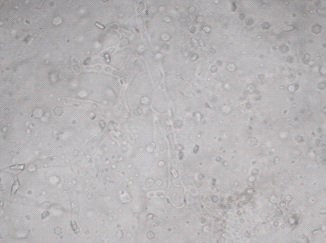
Chest X-ray and MRI of paranasal sinuses with orbit was done. Bilateral lung field appear normal in Chest X-ray. MRI showed mucosal thickening in bilateral maxillary (Red solid arrow), ethmoid, frontal and sphenoid sinuses (Black arrow with red border) and T2W hypointense area noted in left maxillary and bilateral sphenoid Chest X-ray and MRI of paranasal sinuses with orbit was done. Bilateral lung field appear normal in Chest X-ray. MRI showed mucosal thickening in bilateral maxillary (Red solid arrow), ethmoid, frontal and sphenoid sinuses (Black arrow with red border) and T2W hypointense area noted in left maxillary and bilateral sphenoid sinuses. After post contrast it showed necrosis in left maxillary, left ethmoid and bilateral sphenoid sinuses, left middle, inferior nasal turbinates and left side of nasal septum which all suggestive of invasive fungal sinusitis involving left maxilla, left ethmoid and bilateral sphenoid sinuses, left nasal cavity, left side on nasal septum with intra orbital extension (Plain arrow) and involvement of the maxillary alveolararch and hard palate. RT-PCR was negative for COVID-19 on 10th June 2021. KOH wet mount of nasal secretion (Figure 2) showed plenty of broadaseptate branching hyaline fungal hyphae and demonstrates aerial unbranched and branched sporangiophores arising randomly from mycelia. No rhizoids are present and the sporangia are large and spherical. Based on above investigations diagnosis of Rhino-Orbital Mucormycosis was confirmed.
Patient was started on Amphotericin B 60 mg IV OD, Clindamycin 300 mg IV twice BD, Serratiopeptidase Tab 10 mg TDS, Inj. Cefoperazone plus sulbactam 2 gm IV BD. Insulin Glargine 100 IU was started to control hyperglycemia.
Surgical debridement was planned under general anesthesiato clean pus in the affected part and to remove the necrotic tissues. Endoscopic debridement of bilateral paranasal sinuses was done. Left side debridement was done via Denker’s approach. On left side middle turbinate, inferior turbinate, pterygoid plate, posterior part of septum werenecrosed and thus removed. After 1 week of surgery repeat KOH wet mount was sent in which no fungal morphology was seen.
Discussion
It has been noticed that Mucormycosis is complication of COVID-19 disease who have immunocompromised status. COVID-19 disease has a propensity to cause extensive pulmonary disease and subsequent alveolo-interstitial pathology. This by itself may predispose to invasive fungal infections of the airways including the sinuses and the lungs [6]. In Head and Neck cases, the mold usually gains entry through the respiratory tract involving the nose and sinuses, with possible further progression into the orbital and intracranial structures [7]. Study shown that Mucormycosis is present in people who were active (59.4%) or recovered (40.6%) from COVID-19. Pre-existing Diabetes Mellitus (DM) was present in 80% of cases, while concomitant Diabetic Ketoacidosis (DKA) was present in 14.9%. Corticosteroid intake for the treatment of COVID-19 was recorded in 76.3% of cases [8]. Early diagnosis and early treatment with liposomal amphotericin B and surgery are essential for the successful management of Mucormycosis. Thus, the use of glucocorticoids in mild COVID-19 cases (without hypoxemia) or the utilization of higher doses of glucocorticoids should be avoided [9]. Therefore, physician should mindful for probability of development of Mucormycosis in such patients.
Conclusion
Getting Mucormycosis is increased in patient with rampart use of corticosteroid and who have lower immunity. Hyperglycemia should be in control and judicial use of corticosteroids can help to reduce chances for getting rare life-threatening disease. Patient should undergo immediate imaging studies with an emphasis on the requirement of surgical intervention.
References
- healthline.com/health/Mucormycosis. https://www.healthline. com/health/Mucormycosis
- Spellberg B, Edwards J Jr, Ibrahim A. Novel perspectives on mucormycosis: Pathophysiology, presentation, and managemen, Clin Microbiol Rev. 2005; 18: 556-569. https://pubmed.ncbi. nlm.nih.gov/16020690/
- Gleissner B, Schilling A, Anagnostopolous I, Siehl I, Thiel E. Improved outcome of zygomycosis in patients with hematological diseases? Leuk Lymphoma. 2004; 45: 1351-1360. https:// pubmed.ncbi.nlm.nih.gov/15359632/
- Prakash H, Chakrabarti A. Global epidemiology of mucormycosis. J Fungi. 2019; 5: 26. https://pubmed.ncbi.nlm.nih. gov/30901907/
- Skiada Anna, Pavleas Ioannis; Drogari-Apiranthitou Maria. “Epidemiology and Diagnosis of Mucormycosis: An Update” J. Fungi. 2020; 6: 265. https://doi.org/10.3390/jof6040265
- Angneux JP, Bougnoux ME, Dannaoui E, Cornet M, Zahar JR. Invasive fungal diseases during COVID-19: We should be prepared? J Mycol Med. 2020; 30: 100971. https://pubmed.ncbi. nlm.nih.gov/32307254/
- Maini A, Tomar G, Khanna D, Kini Y, Mehta H, Bhagyasree V. Sinoorbital mucormycosis in a COVID-19 patient: A case report. Int J Surg Case Rep. 2021; 82: 105957. https://pubmed.ncbi.nlm.nih. gov/33964720/
- Singh AK, Singh R, Joshi SR, Misra A. Mucormycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab Syndr. 2021; Epub ahead of print. https://www. ncbi.nlm.nih.gov/pmc/articles/PMC8137376/
- Revannavar SM, PSS, Samaga L, et al. COVID-19 triggering mucormycosis in a susceptible patient: A new phenomenon in the developing world? BMJ Case Reports. CP. 2021; 14: e241663. https://pubmed.ncbi.nlm.nih.gov/33906877/