
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Body and tail pancreatic tumor – A rare location: A case report
Crenguta Livia Calma1,2*; Sabine Stefania Groza1
1 Discipline of Physiology, Department of Functional Sciences, “Victor Babeș” University of Medicine and Pharmacy Timișoara, Eftimie Murgu Square No. 2, 300041, Timișoara, Romania.
2 Center of Immuno-Physiology (CIFBIOTEH), “Victor Babeș” University of Medicine and Pharmacy Timișoara, Eftimie Murgu Square No. 2, 300041 Timișoara, Romania.
*Corresponding Author: Crenguta Livia Calma
Discipline of Crenguta Livia Calma Physiology, Department of Functional Sciences, Center of Immuno-Physiology (CIFBIOTEH) “Victor Babeș” University of Medicine
and Pharmacy Timișoara, Eftimie Murgu Square No. 2,
300041 Timișoara, Romania.
Email: crenuguta.calma@umft.ro
Received : Nov 04, 2021
Accepted : Feb 04, 2022
Published : Feb 11, 2022
Archived : www.jcimcr.org
Copyright : © Calma CV (2022).
Abstract
This case report focuses on the body and tail pancreatic tumor, one of the rarest locations of a tumor. We describe an interesting case of thirty-year-old women from a rural region presenting with a giant and a life-threatening pancreatic tumor. The information obtained from the patient revealed a modification of the women’s general condition from the previous two weeks – she presented with fatigue, diffused abdominal pain in the upper abdominal floor, and general condition slightly influenced.
X-ray Computed Tomography Scan (CT scan) with contrast substance (contrast-enhanced Computed Tomography (CT) scan) and Magnetic Resonance Imaging (MRI) both indicate an intense pancreatic body and tail tumor vascularization, well-delimited, solid, with several necrotic areas in the interior, hyper capture in arterial time in the solid portion and wash-out in the portal and parenchymal time, with a size of 6.82 /4.74/6.3 centimeters - T3N0M0, II-A stage.
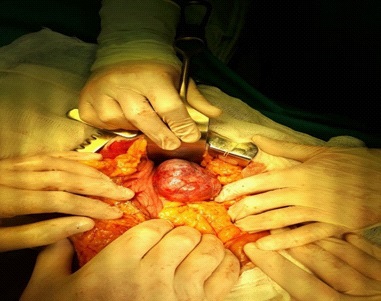
During the surgery, a tumor of approximately 10/7/4.3 centimeters, of firm consistency, irregular shape, encapsulated, lining the posterior gastric face was discovered in the body and tail of the pancreas. On palpation, no adenopathy was detected, and the rest of the abdominal organs have a normal macroscopic appearance. The splenic artery and vein adhere intimately to the tumor and are separated after careful dissection. Subsequently, the splenic hilum is identified, the caudal splenopancreatectomy is decided, performed, and successfully managed.
Keywords: body and tail pancreatic tumor; caudal splenopancreatectomy; pancreatic pseudopapillary neoplasm.
Citation: Calma CV, Groza SS. Body and tail pancreatic tumor – A rare location: A case report. J Clin Images Med Case Rep. 2022; 3(2): 1654.
Introduction
This case report focuses on the body and tail pancreatic tumor, one of the rarest locations of a tumor. Approximately 75% of pancreatic cancers occur in the head (HD) of the pancreas, whereas 15-20% occur in the body and 5-10% occur in the tail (BT) [1,2].
We describe an interesting case of thirty-year-old women from a rural region presenting with giant and a life-threatening pancreatic tumor that was successfully managed.
The medical and social consequences of this type of tumor are found within the general characteristics of the operated tumor diseases.
Case presentation
A 30-year-old woman from a rural region of Western Romania was admitted to hospital on 22 March 2018 with suspicion of pancreatic tumor and peritumoral adherence.
The information obtained revealed a modification of the women’s general condition from the previous two weeks – she presented with fatigue, diffused abdominal pain in the upper abdominal floor and general condition slightly influenced.
The differential diagnoses of hepatitis or gallstones in gallbladder or pseudocysts/cysts and pancreatic abscesses were made.
The physical examination revealed a supple abdomen, painful in the right and left hypochondrium both spontaneously and at palpation and mobile with respiratory movements. In the epigastric region, it is detected at the deep palpation, the presence of a mobile tumor formation, of large size and firm consistency
Intestinal transit and diuresis are present; no signs of peritoneal irritation; the liver and spleen are within normal limits.
X-ray Computed Tomography Scan (CT scan) with contrast substance (contrast-enhanced Computed Tomography (CT) scan) and Magnetic Resonance Imaging (MRI) both indicate a hypervascularization pancreatic body and tail tumor, well-delimited, solid, with several necrotic areas in the interior, hypercapture in arterial time in the solid portion and wash-out in portal and parenchymaltime, with size of 6.82 /4.74/6.3 centimeters; this formation develops extrapancreatic, anterior and inferior, imprinting the posterior wall of the body of the gastric antrum, without invading the splenic vascular package - probably neuroendocrine tumor; without secondary abdominal metastases and without intra-abdominal adenopathy - T3N0M0, II-A stage. The decision of the surgery is made. The xiphosubombilical incision is practiced, the musculo fascial planes are divided thus penetrates into the peritoneal cavity (Figure 1). An aperture is formed by cutting the gastrocolic ligament and entering the omental bursa. Thus, a tumor of approximately 10/7/4.3 centimeters (Figure 2), of firm consistency, irregular shape, encapsulated (Figure 3), lining the posterior gastric face was discovered in the body and tail of the pancreas. On palpation, no adenopathy is detected, and the rest of the abdominal organs have a normal macroscopic appearance. The splenic artery and vein adhere intimately to the tumor and are separated after careful dissection. Subsequently, the splenic hilum is identified, the caudal splenopancreatectomy is decided (the standard treatment for pancreatic body/tail tumors) [3] and performed. It is practiced drainage of the splenic and pancreatic lodge, washing, hemostasis control, closure on anatomical planes with yarn to the skin and then, sterile dressing. The excised piece (pancreatic body and tail) is sent for histopathological examination which shows a solid pseudopapillary epithelial tumor of the pancreas with negative margins.


During the hospitalization, hydroelectrolyte solutions, analgesic, anti-inflammatory, low molecular weight heparin and antiplatelet aggregating were administered.
The post-surgical evolution was favorable, and the patient became afebrile, with an ameliorated appetite and a good general condition. She was discharged from the hospital after two weeks with recommendations for follow-up and oncologic therapy.
Discussion
It is difficult to diagnose a body and tail pancreatic tumor due to nonspecific symptoms and slow evolution over time. The efficient diagnosis of the tumor is based on imaging techniques - CT and MRI [4].
The tumor is difficult to operate due to the anatomical position, an important role in having the experience and specific specialization of the surgeon [5].
Essential is an accurate staging of disease because unresectable tumors are those with distant and vascular metastases. Around 15–20% of patients have respectable disease, but only around 20% of these survive to 5 years.
It has been shown that in establishing the survival prognosis for pancreatic tumors, its location is essential.
Published studies show that the rate of respectability in pancreatic head tumors (HD) is significantly higher than in the pancreatic Body and Tail tumors (BT).
Effective screening methodology is mandatory in pancreatic cancer using sensitive and specific biological markers, along with high resolution imaging methods [6].
Declarations
Funding: This research didn’t receive grants from any funding agency in the public, commercial or not-for-profit sectors.
Conflicts of interest: The authors declare that they have no conflicts of interest and that there were no funding sources.
Guarantor: The guarantor for this paper is Crenguta Livia Calma MD, Ph.D.
Author contributions: CLC proposed the study, performed research and wrote the first draft. SSG performed the research. All the authors were involved in the development of the manuscript and approved the final version.
References
- Kabashi S, Dedushi K, Ramadani N, Mucaj S, Hoxhaj A, Jerliu N. Pancreatic Carcinoma: The Disease that Kills. World J Oncol. 2016; 7: 13-16.
- Barreto S. Tumors of the Pancreatic Body and Tail. World J Oncol. 2010; 1: 52-65.
- Andrén Sandberg Å. Tumors of the body and tail of the pancreas. N Am J Med Sci. 2011; 3: 489-494.
- Mihalache O, Doran H, Poiană C, Birligea A, Cirstea MO, Pătraşcu T. Pancreatic Neuroendocrine Tumors - Case Series and Literature Review. Chirurgia (Bucur). 2019; 114: 630.
- Hajjar NA, Terezia Muresan, Iancu C, Bãlã O, Szasz A, Chiorescu S, Boruah P, Pitu CZF. Diagnostic, atitudine terapeuticã si prognostic în tumorile pancreatice corporeocaudale - prezentare de caz si recenzia literaturii. Chirurgia (Bucur). 2008; 103: 709-714. https://www.revistachirurgia.ro/cuprinsen.php?EntryID=683
- Poruk KE, Firpo MA, Adler DG, Mulvihill SJ. Screening for pancreatic cancer: Why, how, and who? Ann Surg. 2013; 257: 17-26.