
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Osteoid osteoma of the quadrilateral surface of the medial wall of the acetabulum treated with the anterior intrapelvic approach
Hessin Mahmoud1*; Mahmoud Mohamed2; Yehia Ahmed2; Abdelazeem Ahmed3
1Egypt Ministry of Health and Population, Orthopedic Consultant, Egypt.
2Egypt Ministry of Health and Population, Orthopedic Specialist, Egypt Giza Italian District, Egypt.
3Cairo University Kasr Alainy Faculty of Medicine, Egypt Giza Dokki Administration Tower, Egypt.
*Corresponding Author: Hessin Mahmoud
Egypt Ministry of Health and Population, Orthopedic Consultant, Egypt.
Email: drmhessin2010@gmail.com
Received : Dec 02, 2021
Accepted : Feb 07, 2022
Published : Feb 14, 2022
Archived : www.jcimcr.org
Copyright : © Mahmoud H (2022).
Abstract
Acetabular osteoid osteoma is very rare entity. The author reports on a lesion in a 33-years-old lactating female after 12 months of delay in diagnosis. Its periarticular location on the quadrilateral surface of the medial wall and its proximity to the obturator neurovascular bundle made its accessibility by the available minimally invasive treatment options difficult and dangerous. Surgical access through the traditional hip approaches is infeasible. Stoppa intrapelvic approach allowed direct visualization and en bloc resection of the lesion. Pain disappeared immediately after surgery with rapid improvement of her function. Temporary traction obturator neuropraxia was the only complication encountered. Full functional recovery was detected after three months and continued till the latest one-year follow-up with no recurrence manifestations.
Keywords: acetabular osteoid osteoma; hip osteoid osteoma; osteoid osteoma; stoppa approach; quadrilateral; acetabulum osteoid osteoma; nidus.
Citation: Mahmoud H, Mohamed M, Ahmed Y, Ahmed A. Osteoid osteoma of the quadrilateral surface of the medial wall of the acetabulum treated with the anterior intrapelvic approach. J Clin Images Med Case Rep. 2022; 3(2): 1659.
Background
Osteoid osteomas (OOs) represent around 10% of benign bone tumors. It is more common in males, under 30 years of age, with long bones of the lower limbs and spine predominance. Intra-articular lesions are uncommon and represent 5-12% with the hip joint sharing with 13% of which, occurring predominately on the femoral side [1]. In literature, there are mainly sporadic case reports and few small-size case series reporting on acetabular OOs, in different locations, with no agreement on the standard technique for treatment [1-3]. In 2017, Kelly and his colleagues reported on the largest case series identifying ten cases over a period between 2000 and 2015. Over the same period, they identified only 18 prior case reports reporting on a total of 27 cases (single case in thirteen, two cases in three, three and five cases in a single report). The lesion locations were widely variable [1]. Variable conservative and operative treatment modalities were used depending mainly on the OO location, facilities available and physician experience. Successful operative outcomes were reported with open excision, mainly via the safe surgical hip dislocation approach, as well as other minimally invasive options including percutaneous imaging-guided resection and drilling, thermal ablation using radio frequency or laser, and arthroscopic excisions [1-5].
In this account, we describe a case report of acetabular OO located on an atypical site; pelvic (quadrilateral) surface of the medial wall and highlight the challenge in its management decision making.
Case presentation
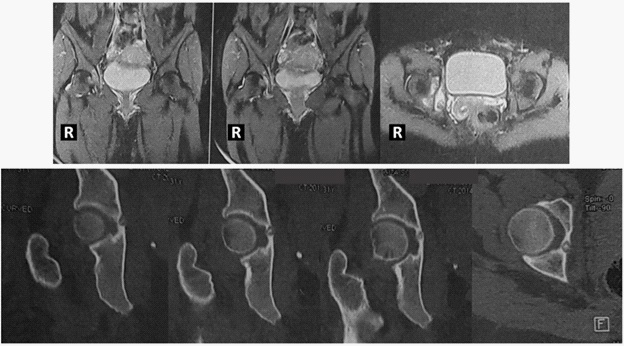
A thirty-three years-old female lactating a one-month-old baby, without significant medical history presented with right groin pain for the past twelve months. On visual analog scale (VAS), the pain ranged from distressing to unbearable pain (five to ten points) especially at night. It is somehow relieved with nonsteroidal anti-inflammatory medications. Clinical examination revealed antalgic gait, non-specific tender point, and painful but full active and passive hip ranges of motion. The laboratory blood tests were normal. Plain radiographs did not show any apparent abnormality. Magnetic resonance imaging (MRI) revealed altered marrow signal of the right acetabulum; eliciting marrow oedema signal of low T1, bright T2 and STIR sequences with surrounding peri-articular fine edematous sheets (Figure 1). The complementary computed tomography (CT) scan revealed an underlying small focally lucent nidus surrounding central sclerotic dot of the osteoid osteoma located on the pelvic side of the medial wall (quadrilateral plate) of the right acetabulum (Figure 1). She scored 56 points on modified Harris hip (mHHS) scoring system.
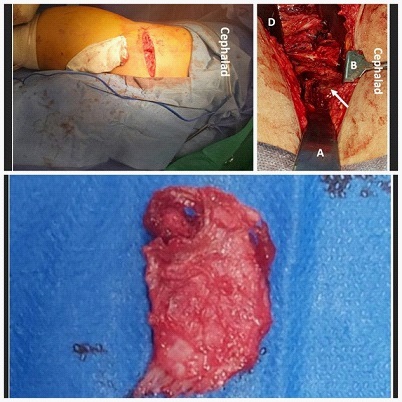
Although the patient had a cesarean delivery one month ago, she insisted on removing the lesion as soon as possible. The decision making and treatment strategy were defined by the lesion site. Under the spinal anesthesia and the supine position, open surgery was done utilizing the same horizontal skin incision of the cesarean section and the anterior intrapelvic Stoppa approach (Figure 2). With the surgeon standing on the opposite side of the lesion, the rectus fascia was split longitudinally along the line a alba, followed by elevation and retraction of the ipsilateral rectus abdominis muscle. Ligation of the abnormal obturator vein (venous corona mortis) followed with gentle retraction of the main obturator neurovascular bundle and the peritoneum allowed full exposure of the medial surface of the innominate bone (quadrilateral plate) below the pelvic brim with direct visualization of the lesion (Figure 2). En bloc resection of the lesion was done using a curved osteotome removing part of the inner table of the medial acetabular wall (Figure 3). This did not allow exposure of the joint cavity nor the femoral head. The operation time was 45 minutes with minimal blood loss and no complications.
On the second postoperative day, the patient fortunately reported dramatic improvement and almost disappearance of the agonizing night pain. She was discharged from the hospital on the third day after removal of the drain. Pathological analysis of the specimen confirmed the diagnosis. After two weeks, the wound was checked and exposed. The patient had minor limping and reported not using any analgesics after the tenth postoperative day. Ipsilateral hip muscles power examination revealed; weakness (grade 2/5) of the adductors and full strength of the flexors, extensors, and abductors. She was referred for the physical therapy for muscles strengthening program.
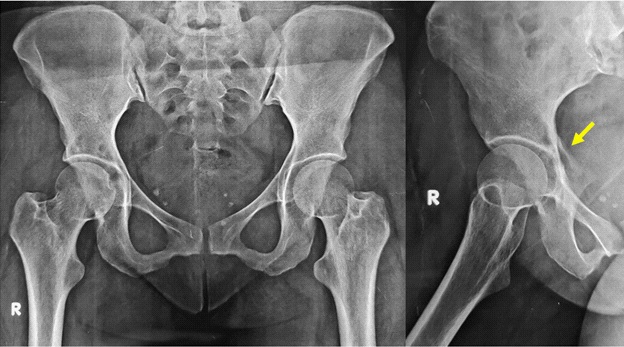
At three months, no limping was detected, and adductors regained full strength. No pain on VAS score and excellent modified Harris hip score (100 points). X-rays showed full consolidation of the defect on the quadrilateral surface (Figure 4). The same findings were maintained till the latest follow up at one year with no recurrence of the manifestations.
Discussion
Acetabular osteoid osteoma is very rare entity presenting with atypical symptoms and signs coinciding with other more common hip diseases. Moreover, generally the intra-articular lesions give atypical radiographic picture different from the traditional extra-articular type, without the obvious surrounding sclerosis. These reasons make its diagnosis a challenge leading to frequent wrong interpretation and delayed diagnosis [1,2]. This case had several diagnostic challenges; atypical age group, female gender, and the pregnancy. She reported suffering from the OO pain 2 months before knowing that she was pregnant, however this pain was interpreted wrongly during this period and during pregnancy as related to an obstetric cause, that should be disappear with the delivery. Two weeks after the delivery, MRI was ordered for suspicion of the commonly encountered diseases seen in this patient type namely transient osteoporosis of the hip or stress fractures. However, the MRI signals and the complementary CT scan showed the typical lesion of OO (Figure 1).
The natural history of the OO is spontaneous resolution within five to seven years, with earlier pain relieve at an average of three years. However, conservation with clinical observation and non-steroidal anti-inflammatory drugs (NSAIDs) usually fails due to two major reasons: the intolerable degree of the persistent pain caused by the high local concentration of prostaglandin E2, and the intolerance of the side effects caused by long term treatment by the NSAIDs [2]. In this case, the patient insisted on interventional treatment immediately after reaching a definite diagnosis. She was unable to stand further years of pain, nor tolerating the gastric upset caused by the drugs.
Several interventions had been reported in literature depending on many factors, mainly the location of the lesion in the acetabulum [1-5]. Most recently, Efthymiad is and his colleagues investigated in a systematic review and proportional meta-analysis the ideal minimally invasive technique for treatment of hip OO. They concluded that radiofrequency ablation (RFA) and arthroscopic excision could be most effective treatment options. Reported major complications; factures and deep infection and minor complications; transient paraesthesia, intermuscular hematomas and wound burn occurred with CT- guided RFA, however no complications were reported with the arthroscopy. They highlighted the importance of individualization and tailoring the treatment options according to the lesion, equipment available and physician expertise [1]. In this case, its location on the medial acetabular wall made it difficult to access by RFA that produce an average of one-centimeter zone of heat necrosis. This may risk the pelvic cavity vessels and nerves, especially the obturator neurovascular bundle which cross the pelvic cavity from the greater sciatic notch, in close contact with the medial acetabular wall and quadrilateral plate, to reach the obturator foramen anteriorly. Another concern is the articular cartilage thermal damage and premature degenerative changes previously reported in the acetabulum and other periarticular locations [3]. Similarly, its location on the pelvic side (Figure 1) made it difficult to access by arthroscopy. We thought that the only pathology that might be seen from the joint side was inflammatory changes that may be indecisive and confusing. This may carry a high risk of not hitting the desired nidus target or producing an undesired articular cartilage damage. Another concern was the technical complexity of the hip arthroscopy procedure.
Open surgical resection was the procedure of choice in our opinion. Preoperative planning necessitates the use of an intrapelvic approach to be able to see and excise the lesion directly without any joint damage. We used the Stoppa approach, usually used for acetabular fractures management, consuming the same horizontal skin incision of the delivery. This allowed full exposure of the quadrilateral plate and the lesion after ligation of the corona mortis (Figure 2). En bloc resection required gentle retraction of the obturator neurovascular bundle. We assume that this was the reason for the obturator neuropraxia leading to the temporary hip adductors weakness postoperatively.
The acetabulum is a rare location for OO lesions. Moreover, the location on the quadrilateral surface of the medial wallis peculiar and unique. Its accessibility without complications is challenging. Stoppa intrapelvic approach allowed easy and direct accessibility to the lesion as well as safe resection.
References
- Efthymiadis A, Tsikopoulos K, Uddin F, Kitridis D, Edwards N, Sidiropoulos K, et al. Which is the optimal minimally invasive treatment for osteoid osteoma of the hip? A systematic review and proportional meta-analysis. Journal of orthopaedic science: official, journal of the Japanese Orthopaedic Association. 2021. S0949-2658(21)00013-0. Advance online publication. https://doi.org/10.1016/j.jos.2020.12.026
- Spiker AM, Rotter BZ, Chang B, Mintz DN, Kelly BT. Clinical presentation of intra-articular osteoid osteoma of the hip and preliminary outcomes after arthroscopic resection: a case series. Journal of hip preservation surgery. 2017; 5(1): 88-99.
- Bosschaert PP, Deprez FC. Acetabular osteoid osteoma treated by percutaneous radiofrequency ablation: delayed articular cartilage damage. JBR-BTR: organe de la Societeroyalebelge de radiologie (SRBR) = orgaan van de KoninklijkeBelgischeVerenigingvoorRadiologie (KBVR). 2010; 93(4): 204-206.
- de Los Santos O, Filomeno P, Rey R, Cúneo, A. Acetabular osteoid osteoma excision by controlled hip dislocation: a case report. Journal of pediatric orthopedics. Part B. 2013; 22(3): 195-199.
- Marwan YA, Abatzoglou S, Esmaeel AA, Alqahtani SM, Alsulaimani SA, Tanzer M, et al. Hip arthroscopy for the management of osteoid osteoma of the acetabulum: a systematic review of the literature and case report. BMC musculoskeletal disorders. 2015; 16: 318.