
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Megagiant liver hemangioma: A case report of rare entity
Nikhil Shellagi*; Hirak Pahari; Barun Nath; Udipta Ray
Department of Surgical Gastroenterology and Liver Transplantation, Medica Hospital, Kolkata, India.
*Corresponding Author: Nikhil Shellagi
Department of Surgical Gastroenterology and Liver Transplantation, Medica Hospital, Kolkata, India
Email: nikyshellagi@gmail.com
Received : Nov 02, 2021
Accepted : Feb 08, 2022
Published : Feb 15, 2022
Archived : www.jcimcr.org
Copyright : © Shellagi N (2022).
Abstract
Hemangioma is the most common neoplasm of the liver, affecting 0.4-20% of the general population. The incidence of hemangiomas is highest in the third to fifth decade of life and is more common in women. Most hemangiomas are asymptomatic and diagnosed incidentally. Hemangiomas with diameter more than 5 cm in size is termed Giant Hemangioma. Symptomatic giant hemangiomas with severe incapacitating symptoms, consumptive coagulopathy, diagnostic uncertainty, rapid growth and complications such as bleeding and rupture, are the most indications for surgical treatment. Here we present a case of symptomatic megagiant hemangioma. There are few case reports and small case series of large giant hemangioma published in the literature.
Citation: Shellagi N, Pahari H, Nath B, Ray U. Megagiant liver hemangioma: A case report of rare entity. J Clin Images Med Case Rep. 2022; 3(2): 1660.
Introduction
Hemangiomas are the most common benign tumor of the liver with an estimated prevalence of 0.4% to 20% [1]. Majority of these patients are asymptomatic, these lesions are usually detected incidentally through the increased use of imaging method for abdominal complaints. A hemangioma with a diameter of more than 5 cm is termed giant hemangioma [2]. Giant hemangiomas can become symptomatic and even may cause complications such as mechanical complications and coagulopathy [3]. Symptomatic giant hemangiomas with severe incapacitating symptoms, consumptive coagulopathy, diagnostic uncertainty, lesion growth and complications as bleeding and rupture, are the indications for surgical treatment [4,5]. Discussion about the management of giant liver hemangiomas with diameter greater than 20 cm is scarce.
Case report
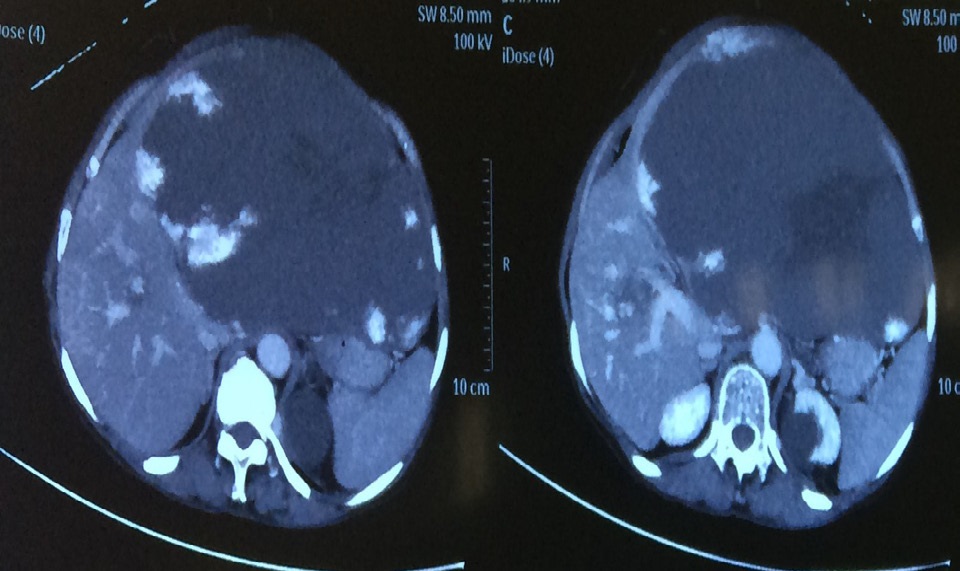
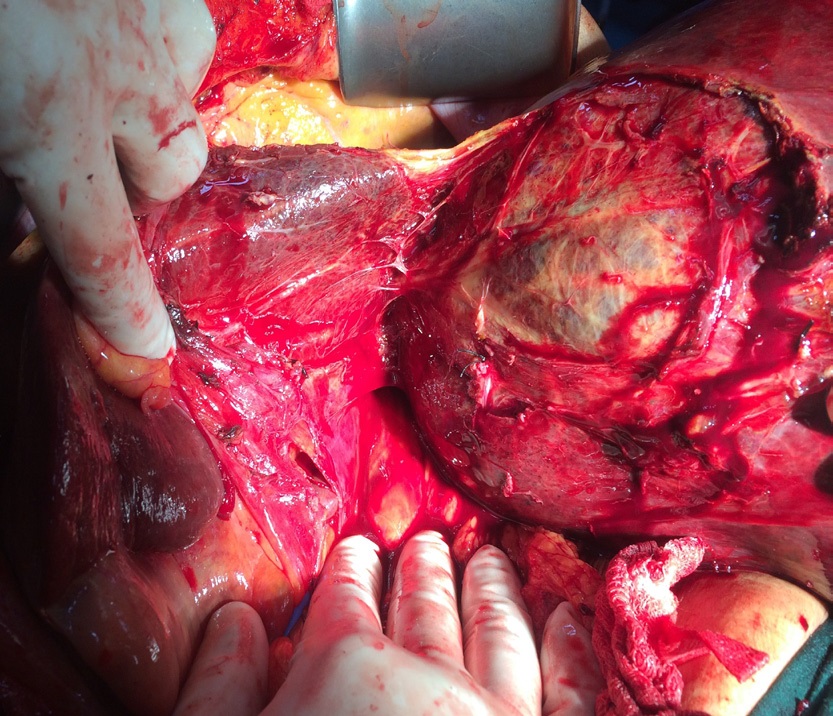
A 53 year old female patient from North Eastern region of India presented to us with history of progressive abdominal distension and generalised abdominal pain of six months duration. She had no other associated symptoms. General physical examination was unremarkable and abdominal examination revealed large mass (20 X 25 cm) with well defined borders inferiorly and laterally. Blood work up was essentially normal except mildly deranged coagulation profile. CECT Abdomen revealed large hemangioma in left lobe and few small hemangioma in the right lobe. In view of large size of hemangioma and anticipated major bleeding during surgery. Pre operative super selective angioembolisation of feeder vessels was done using PVA. Post embolisation period was eventful. She was taken up for surgical resection after 2 days. Left lateral segmentectomy with enucleation of hemangioma in the right lobe was done. The total duration of surgery was around 180 minutes with estimated blood loss around 150 ml. Intra operative and post operative period was uneventful. Patient was discharged on post operative day 5. Coagulation profile normalised in the post operative period. The probable reason was consumptive coagulopathy (Due to large size of hemangioma). Histopathological examination revealed well capsulated lesion with 25 X 24 X 10 cm dimension and weighed 4.5 kg was suggestive of hemangioma. Patient was followed up at third month, she was asymptomatic and blood work up was normal and no abnormality was detected on imaging.
Discussion
Liver hemangioma occurs more frequently in women than in men, and is believed to be related to levels of female hormones [6]. Most liver hemangiomas remain stable in size. It has been proposed that asymptomatic patients with hemangiomas less than 5 cm require no intervention therapy. Also, the patients with giant hemangiomas with no symptoms can be observed safely without the chance of developing complications [7]. Schnelldorfer et al reported that clinical observation is prefered in most patients with giant hemangioma in a recent retrospective cohort study [8]. The occurrence of spontaneous rupture is rare, even in giant hemangiomas [9]. However our patient had progressive abdominal pain associated with abdominal distension. The indications of surgery for giant hemangioma are well defined. Symptomatic giant hemangioma with abdominal pain and discomfort not controlled by medical treatments is commonly the major indication for surgery [10]. Hemangioma size is usually stable and reported increase in size varied from 8,7 to 14% [11] and a minimum of 25% increase in largest diameter over a period of 6 months was defined as a rapid growth justifying indication of surgery for asymptomatic hemangiomas [12]. Consumptive coagulopathy or Kasabach-Merritt syndrome requires a surgery, but its incidence is extremely rare [10].
Technical aspects of surgical treatment may vary greatly between centers. Hepatic resection and enucleation are the most commonly used surgical procedures to treat surgically liver hemangiomas [10]. The enucleation is preferred by some authors because there is a dissection plane between hemangioma and liver parenchyma making transversing vessels ligation much simpler decreasing the risk of blood loss, and the risk of postoperative bile leak is much lower due to the absence of bile ducts in the enucleation dissection plane. Also, enucleation preserves the healthy liver parenchyma avoiding unnecessary parenchyma loss for the treatment of benign tumor [13]. Compared to peripherally located hemangiomas, enucleation of centrally located hemangiomas is more likely associated with longer operative time and higher rate of blood loss and transfusion [14]. Hamaloglu et al reported enucleation should be considered in the case of anterior and superficial hemangiomas [15].
Recently reported, the risk of bleeding and blood transfusions is to be more related to hemangioma size than to the type of surgical technique [11]. Furthermore, evolution toward enucleation over resection even for large hemangiomas over time with less blood loss and transfusions and less complications have been documented and reported [16]. Hepatic resection and enucleation of giant hemangioma are associated with similar rate of blood loss and transfusions [11]. Furthermore, the risk of bleeding and blood transfusions was more related to tumor size [11] and blood transfusion was more needed in patients with hemangiomas larger than 10 cm in size [17]. When indicated, liver resection for hemangiomas can be performed safely with low morbidity and nil mortality rates [11,18].
Different treatment modalities of liver hemangiomas apart from resection have been described, such as ligation of hepatic artery [19] or liver transplantation for giant unresectable lesions [20]. Selective transcatheter arterial embolization, RFA and radiation therapy have also been reported [21]. Hepatic artery ligation advocated for unresectable tumors, has been shown to arrest the growth of some lesions This method has disadvantages including limited experience and its ineffectiveness in some patients. So, in the era of “safe” liver surgery, hepatic artery ligation should no longer be recommended [22]. Trans arterial embolization has been used as an alternative treatment for symptomatic hemangiomas [23]. A reduction of symptoms may be possible, but tumor size remains stable after the procedure and recurrence is common. Transarterial embolization preoperatively reduces vascular inflow and decreases size in very large tumors making surgical resection less risked [24]. Radiofrequency ablation has also been used to control symptomatic giant hemangiomas with promising results [11]. The use of RFA in lesions with diameter higher than 10 cm had a very high rate of complications (100%) including life-threatening complications (lower esophageal fistula and acute respiratory distress syndrome) suggesting its inappropriate use in lesions larger than 10 cm [11].
Conclusion
The indications of surgery for giant hemangioma are well defined and surgical approach is widely accepted in symptomatic giant hemangiomas. The symptom development is the most often indication for surgical resection. Surgical management is required for hemangioma complications such as Kasabach Merritt syndrome or consumptive coagulopathy and rupture or bleeding. Pre operative selective transarterial embolization reduces size of hemangioma and decreases bleeding during surgery. Surgical intervention both liver resection and enucleation can be employed to resect giant liver hemangiomas with low morbidity and mortality rates.



References
- Coumbaras M, Wendum D, Monnier-Cholley L, Dahan H, Tubiana JM, Arrivé L. CT and MR imaging features of pathologically proven atypical giant hemangiomas of the liver. AJR Am J Roentgenol. 2002; 179: 1457-1463.
- Adam YG, Huvos AG, Fortner JG. Giant hemangiomas of the liver. Ann Surg. 1970; 172: 239-245.
- Weimann AG, Ringe B, Klempnauer J, et al. Benign liver tumors: Differential diagnosis and indications for surgery. World J Surg. 1997; 21: 983-90.
- Erdogan GD, Busch OR, Van Delden OM, et al. Management of liver hemangiomas according to size and symptoms. J Gastroenterol Hepatol. 2007; 22: 1953-958.
- Hoekstra LT, Bieze M, Erdogan D, et al. Management of giant liver hemangiomas: An update. Expert Rev Gastroenterol Hepatol. 2013; 7: 263.
- Tuncer I, Arslan H, Harman M. Two giant cavernous hemangioma caused cavernous transformation of the portal vein in a pregnant woman. Turk J Gastroenterol 2002; 13: 229-231.
- Farges O, Daradkeh S, Bismuth H. Cavernous hemangiomas of the liver: are there any indications for resection? World J Surg. 1995; 19: 19-24.
- Schnelldorfer T, Ware AL, Smoot R, Schleck CD, Harmsen WS, Nagorney DM. Management of giant hemangioma of the liver: resection versus observation. J Am Coll Surg. 2010; 211: 724-730.
- Corigliano N, Mercantini P, Amodio PM, et al. Hemoperitoneum from a spontaneous rupture of a giant hemangioma of the liver: report of a case. Surg Today. 2003; 33: 459-463.
- Abdelkader Boukerrouche. Management of giant liver hemangioma. J Gastroenterol Dig Dis. 2017; 2: 64-68.
- Yedibela S, Alibek S, Müller V, et al. Management of hemangioma of the liver: Surgical therapy or observation? World J Surg. 2013; 37: 1303.
- Herman P, Costa MLV, Machado MAC, et al. Management of hepatic hemangiomas: A 14-year experience. J Gastrointest Surg. 2005; 9: 853.
- Fu XH, Lai EC, Yao XP, et al. Enucleation of liver hemangiomas: Is there a difference in surgical outcomes for centrally or peripherally located lesions? Am J Surg. 2009; 198: 184-87.
- Aldrighetti L, Cipriani F, Ratti F, et al. The Italian experience in
- Aldrighetti L, Cipriani F, Ratti F, et al. The Italian experience in minimally invasive surgery of the liver: A national survey. In: Calise F, Casciola G (eds) Minimally invasive surgery of the liver, Updates in surgery. Springer, Milan, Rome. 2013.
- Hamaloglu E, Altun H, Ozdemir A, Ozenc A. Giant liver hemangioma: therapy by enucleation or liver resection. World J Surg 2005; 29: 890-893.
- Acharya M, Panagiotopoulos N, Bhaskaran P, et al. Laparoscopic resection of a giant exophytic liver haemangioma with the laparoscopic Habib 4 × radiofrequency device. World J Gastrointest Surg. 2012; 4: 199.
- Yamagata M, Kanematsu T, Matsumata T, et al. Management of haemangioma of the liver: Comparison of results between surgery and observation. Br J Surg. 1991; 78: 1223.
- Miura JT, Amini A, Schmocker R, et al. Surgical management of hepatic hemangiomas: A multi-institutional experience. HPB. 2014; 16: 924.
- Nishida O, Satoh N, Alam AS, Uchino J. The effect of hepatic artery ligation for irresectable cavernous hemangioma of the liver. Am Surg. 1988; 54: 483-486.
- Russo MW, Johnson MW, Fair JH, Brown RS Jr. Orthotopic liver transplantation for giant hepatic hemangioma. Am J Gastroenterol. 1997; 92: 1940-194.
- Giavroglou C, Economou H, Ioannidis I. Arterial embolization of giant hepatic hemangiomas. Cardiovasc Intervent Radiol. 2003; 26: 92-96.
- Fu XH, Lai EC, Yao XP, et al. Enucleation of liver hemangiomas: Is there a difference in surgical outcomes for centrally or peripherally located lesions? Am J Surg. 2009; 198: 184-87.
- Zhou JX, Huang JW, Wu H, et al. Successful liver resection in a giant hemangioma with intestinal obstruction after embolization. World J Gastroenterol. 2013; 19: 2974.
- Gao J, Ke S, Ding X, et al. Radiofrequency ablation for large hepatic hemangiomas: Initial experience and lessons. Surgery. 2013; 153: 78.