
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
N-butyl-2-cyanoacrylate renal stone, a rare complication after embolization of urinary fistula: A case report
Angela Costanzo1*; Gabriele Tulone1; Rosa Giaimo1; Antonino Giulio Giannone2; Nicola Pavan3, Marco Vella1; Alchiede Simonato1
1Department of Surgical, Oncological and Stomatological Sciences, Section of Urology, University of Palermo, Palermo, Italy.
2Department of Health Promotion, Mother and Child Care, Internal Medicine and Medical Specialties, Unit of Anatomic Pathology, Italy.
3Urology Clinic, Department of Medicine, Surgery and Health Sciences, University of Trieste, Trieste, Italy.
*Corresponding Author: Angela Costanzo
Department of Surgical, Oncological and Stomatological Sciences, Section of Urology, University of Palermo, Palermo, Italy.
Tel: 339-184-6631;
Email: angelacostanzo87@gmail.com
Received : Jan 04, 2022
Accepted : Feb 08, 2022
Published : Feb 15, 2022
Archived : www.jcimcr.org
Copyright : © Costanzo A (2022)..
Abstract
Embolization with N-butyl-2-cyanoacrylate (NBCA) is an effective and safe procedure recently used for closure of upper tract urinary fistula. However, NBCA constitutes a foreign body for human organs, so it can cause complications. In our case a 56-year-old man underwent an endoscopic embolization of urinary fistula with NBCA. Six years later an UroCT scan revealed a large lithiasis of the left kidney, treated with endoscopic and percutaneous surgery. Stone analysis revealed a composition of crystals mixed with cyanoacrylate. In our opinion this example of complication after NBCA use for endoscopic procedures, rarely reported in literature, can be an useful advisement to reconsider the use of this glue.
Keywords: N-butyl-2-cyanoacrylate; gluestone; percutaneous; endoscopic; fistula
Citation: Costanzo A, Tulone G, Giaimo R, Giannone AG, Pavan N, et al. N-butyl-2-cyanoacrylate renal stone, a rare complication after embolization of urinary fistula: A case report J Clin Images Med Case Rep. 2022; 3(2): 1662.
Introduction
Use of N-Butyl-2-cyanoacrylate (NBCA) to repair urinary leakage is a non-invasive procedure, recently increasingly reported. It is generally safe and effective. However, it is not totally safe and some complications from these treatment are reported. Despite its properties of biocompatibility, NBCA is a foreign body for human organs with a slowly in vivo degradation. In this article, we reported a case of rare complication after urinary fistula’s embolization with NBCA causing the formation of a cyanoacrylate core stone.
Case report
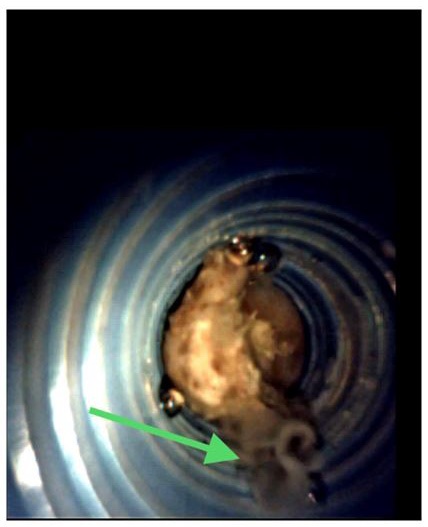
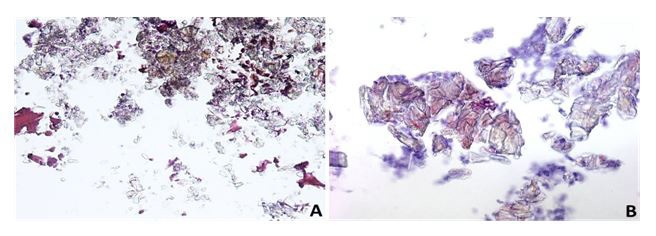
A 56-year-old man, without a medical history of lithiasis, underwent an uncomplicated left lower pole laparotomic partial nephrectomy for Fuhrman grade 2 pT1bNxMx clear cell renal cell carcinoma in 2014. During the postoperative period, he developed a fistula that was managed conservatively with an endoscopic embolization with NBCA in a different center. In the following period, an imaging follow-up demonstrated a proper repair of the upper urinary tract. After six years, an ultrasound showed an hyperechoic image in the left kidney referred to cyanoacrylate residual, confirmed by an URO-CT scan. A large lithiasis (about 4 cm in diameter) of the inferior and middle left renal calyx partially extending to pelvi was reported. Its radiopacity according to Hounsfield scale was heterogenous, varying from 300 to 1000 units. We treated the patient with 2 steps retrograde intrarenal surgery. During the first procedure the stone was apparently calcific with an easy possibility of fragmentation. However, during the second step an amorphous core appeared, and the stone was appearing filamenteuse and viscose (Figure 1). The fragmentation resulted difficult both with holmium laser and ballistic technique and a percutaneous approach was planned. Using the LithoClast Trilogy lithotripter (combining ballistic with ultrasonic energy and suction) a complete stone removal was achieved. A chemic-physical together with a microscopic analysis of a stone’s fragment (Figure 2) was performed. The analysis reported a tissue fragment with extensive regressive phenomena comprising refracting amorphous material compatible with synthetic glue as NBCA (Figure 3).


Discussion
Urinary leakage is one of the major complications of partial nephrectomy. Its treatment is generally proper conservative management or, alternatively, the placement of a long-term retrograde ureteral catheter. In case of failure, we have to consider the presence of a permanent urinary fistula [1]. A well described alternative treatment is the use of a relatively novel technique with tissue-adhesive materials as NBCA. This synthetic glue is recently increasingly used for endoscopic and percutaneous procedures, especially vascular ones, as embolization. It has many properties that make it very suitable for this use: it is adhesive, hemostatic, antibacterial, it has a good biocompatibility, working well in wet environment with a short polymerization time. Low quantity can be applied with good results [2]. It is usually added to agents as Iophendylate or Tantalum powder in order to augment its radiopacity making its use more feasible with a fluoroscopic guide [3]. Despite best efforts, after NBCA deposition some complications are noted, especially during its use for vascular embolization [4].
Furthermore, NBCA is a foreign body with a long resorption time, so it can constitute an ideal substrate for the processing of nucleation, growth, and aggregation, involved in lithogenesis, especially when the material is applied in a confined site as the renal pelvis. Cesare Selli et al [5] reported the case of a cyanoacrylate cast found in the upper calyx of a patient treated with this glue. In our case, a patient without history of renal lithiasis has become a rare example of developing of a calyceal-pyelic glue-stone as complication after NBCA’s renal application. His medical history, temporal consecution of diagnostic-therapeutic procedures, stone’s aspect, especially the presence of a calcific coating around an amorphous core, intraoperative technical difficulties (the ineffectiveness of an endoscopic approach with holmium laser and the need of a percutaneous one with a trilogy device), radiological image (Figure 4) and pathological analysis corroborate our thesis.
In our opinion this case can be an advisement to re-consider the use of NBCA: intraoperatively, it would be appropriate to do an accurate evaluation of the amount of used glue, to avoid an excessive and unnecessary application and a careful check of caliceal cavities will ensure the absence of residual fragments of NBCA. Postoperatively it can be useful to do an ultrasound follow up to exclude eventual formation of glue’s aggregate.
Acknowledgment: An informed consent was obtained from the patient.
References
- Nouri YM, Chu HH, Shin JH, Tsauo J, Kim CS, Hong BS et al. Percutaneous Obliteration of Urinary Leakage after Partial Nephrectomy Using N-Butyl-Cyanoacrylate Obliteration of the Urinoma with or without Coil Embolization of the Fistula Tract. J Vasc Interv Radiol. 2019; 30(12): 2002-2008.
- Muto G, D’Urso L, Castelli E, Formiconi A, Bardari F. Cyanoacrylic glue: a minimally invasive nonsurgical first line approach for the treatment of some urinary fistulas. J Urol. 2005; 174(6): 2239-43.
- Labby ZE, Chaudhary N, Gemmete JJ, Pandey AS, Roberts DA. Dosimetric measurements of an n-butyl cyanoacrylate embolization material for arteriovenous malformations. Med Phys. 2015; 42(4): 1739-44.
- Hill H, Chick JFB, Hage A et al. N-butyl cyanoacrylate embolotherapy: techniques, complications, and management. Diagn Interv Radiol. 2018; 24(2): 98-103.
- Selli C, De Maria M, Manica M, Turri FM, Manassero Francesca. Minimally invasive treatment of urinary fistulas using N-butyl-2-cyanoacrylate: a valid first line option. BMC Urol. 2013; 13: 55.