
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Lumbar disc herniation in patient with long-term postural in stabilty from achilles tendon rupture: A single case study
Franchini M1*; Giorgetti J2; Formica A3; Casarosa S3
1 Institute of Clinical Physiology, National Research Council, 56124 Pisa, Italy
2 Neurosurgery, Azienda Ospedaliera Pisana, 56126 Pisa, Italy.
3 San Rossore Sport Village SrL, 56122 Pisa, Italy.
*Corresponding Author: Franchini Michela
Institute of Clinical Physiology, National Research
Council, Via Moruzzi, Pisa, Italy
Email: michela.franchini@ifc.cnr.it
Received : Dec 21, 2021
Accepted : Feb 09, 2022
Published : Feb 16, 2022
Archived : www.jcimcr.org
Copyright : © Franchini M (2022).
Abstract
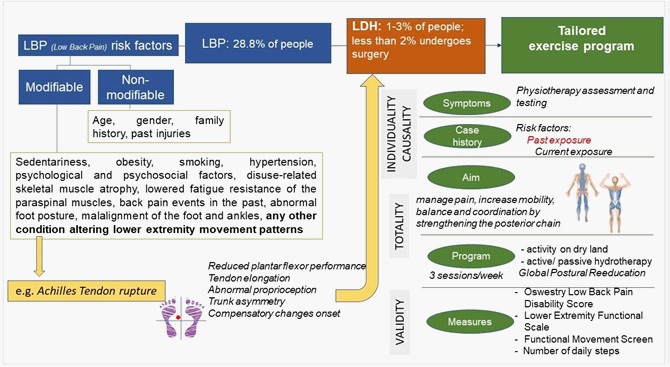
Lumbar Disc Herniation (LDH) may be triggered by many factors acting on the posterior kinetic chain as foot posture, foot and ankles malalignment and abnormal proprioception. Achilles Tendon (AT) rupture can impact heel position, ankle biomechanics, proprioceptive regulation and promote postural instability. This single case study aims to highlight the long-term effects of AT rupture, and its unefficient rehabilitation, on trunk asymmetry that could lead to lumbar degenerative diseases. This study describes a 50 year old woman with long-term postural instabilty from past AT rupture, who undergone to surgery for LDH and physioteraphy. The tailored exercise program included three sessions/week of both physical activity on dry land and active/passive aquatic physiotherapy. Average number of daily steps performed along the patient’s diagnostic and therapeutic pathway has been used to compare the activity rate over time. The Functional Movement Screen, the Owestry Low Back Pain Disability and the Lower Extremity Functional scales have been used as main outcome measures. This work aims to propose an integrated approach to patients with LDH built (a) following the principles of individuality, causality and totality and (b) combining activities on dry land and hydrotherapy within the same physical session, to improve the efficacy of rehabilitation programmes for spine injuries.
Keywords: lumbar disc herniation; achilles tendon rupture; low back pain; individuality; causality; totality.
Citation: Franchini M, Giorgetti J, Formica A, Casarosa S. Lumbar disc herniation in patient with long-term postural in stabilty from achilles tendon rupture: A single case study. J Clin Images Med Case Rep. 2022; 3(2): 1666.
Introduction
Lumbar disc herniation (LDH) is a localized displacement of intervertebral disc tissue beyond the physiological margins of the intervertebral disc space. LDH affects about 1–3% of people, in particular those aged between 30 and 50 years [1]. LDH symptoms include Low Back Pain (LBP), muscle spasm or cramping, leg pain and weakness, sciatica, impairment of leg function and abnormal gait [1]. Back pain episodes in the past are the strongest predictors for back pain in the future and LBP could also be a sign of LDH process, even though some studies found that disc herniation was actually common in asymptomatic people as well [2]. Of all patients who experience episodes of back pain, fewer than 2% will undergo surgery for suspected disc herniation and the correlation between disc degeneration severity and LBP incidence is not linear [2]. LBP may be triggered by a great variety of factors. Changes in lifestyle and in the way of working, such as the intensive use of computer and other tehnologies at work and at home, have increased sedentariness– a risk factor for chronic and acute low back pain due to muscle weakness. Other several factors related to lifestyle - e.g. obesity, smoking, hypertension- are known risk factor for LBP [3]. Psychological and psychosocial factors are further determinats [4]. Furthermore, it has been reported that patients with severe chronic LBP show signs of disuse-related skeletal muscle atrophy and a higher rate of conversion of slow twitch oxidative (type I) fibers towards more vulnerable fast twitch glycolytic fibers (type IIB), compared to healthy people [5]. This may lead to lowered fatigue resistance of the paraspinal muscles which results in higher vulnerability of the lumber spine. LBP is also associated with signs of generalized musculoskeletal hyperalgesia from central sensitization which results from changes in the properties of neurons in the central nervous system, rather than from the presence, intensity, or duration of noxious peripheral stimuli as it happens in acute nociceptive pain [6,7]. People with chronic musculoskeletal pain conditions, such as knee osteoarthritis and subacromial pain syndrome show similar symptoms [6,7]. Altered central pain processing has also been detected in people 48 with Achilles tendinopathy [8,9]. Abnormal foot posture and function have been highlighted as directly associated to the development of LBP [10,11]. The Framingham Foot Study indicates that pronated foot function is significantly associated with LBP in women after adjusting for age, weight, smoking and depressive symptoms [11]. This association may be at least partly explained by the kinematic interaction of the lower extremity joints during walking (calcaneus, talus, tibia, femur and sacroiliac joint) and their influence on the pelvic alignment [12]. Malalignment of the foot and ankles, which determines an unilateral change of the body scheme, may result in compensatory changes of posture for keeping the Center Of Mass (CoM) within the Center Of Pressure (CoP) [10]. Compensatory changes may also result from a unilateral Achilles tendon rupture. There is evidence that a past Achilles Tendon (AT) rupture persistently alters lower extremity movement patterns beyond the ankle, likely as compensation for reduced plantar flexor performance [13,14]. Soleus and gastrocnemius act as active agonists and prevent forward falling of the bodily CoM. Additionally, muscle sensory organs, the spindles and the Golgi tendon organs, play a key role in the proprioceptive regulation of movement [15]. The gastrocnemius muscle is active in walking, jumping, and running, and therefore it is predominantly composed of type II fiber, more involved with exercise of higher intensity and force production [16,17] while the soleus muscle has a stabilization effect on the foot for standing [16,17]. Permanent impairment in plantar flexors performance [18,19] contributes to reduce plantar flexors force production and endurance within the gait cicle [19,20] as well as to impact the ability to perform tasks requiring rapid force production in end67 range plantar flexion [18,19]. Tendon elongation is a futher long-term structural complication of the AT rupture [21] and it may be an important clinical prognosticator of ankle biomechanics, whereas individuals who experienced AT rupture walk with a 15% deficit in ankle power production, and an 18% deficit during the higher-demand task of hopping [22]. As the incidence of acute AT ruptures is increasing [13], this single case study aims to highlight the long-term effects on trunk asymmetry and compensatory changes onset that could lead to lumbar degenerative diseases. It also aims to show how the lack of an early functional rehabilitation protocol for AT rupture can impact the efficiency of future physioteraphy interventions. Furthermore, this work aims to highlight the added value of performing cohmprensive and multidisciplinary evalutaion of the body in its entirety, as the central step in building tailored rehabilitation programs (Figure 1).
Case presentation
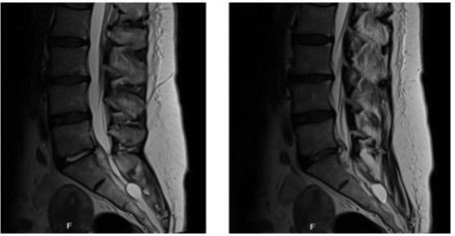
The patient is a 50 year-old woman who firstly presented for a neurosurgical visit in Febraury 2021, with a previous orthopedic report of bilateral acute sacroiliitis. The patient presented with an evident left lateral pelvic tilt, lumbar pain, discomfort in the buttock area and a quite complete inabilty to stand and walk. Lumbar pain and difficulty walking arose four days after her last mild physical activity session. During the previous ten days, she had already been treated with 16 mg/day of Methylprednisolone and 20 mg/day of natural opium alkaloids. The MR report of Febraury 2021 showed a coarse median hernial formation between L5 ans S1 that broke through the annulus fibrosus, migrating in a distal subligamentous position. The expelled material was partly linked to the herniated disk (Figure 2).
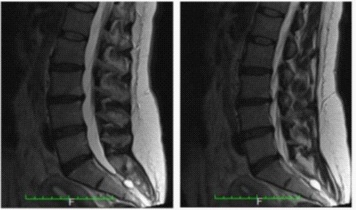
Previous MR reports (years 2010 and 2015) showed a general impaired condition of the back with signs of discs degeneration and osteophyte formations at the cervical, thoracic and lumbar levels. Signs of sub ligamentous herniation of the L5-S1 disk had already been detected in 2010 and annular fissure has been highlighted in April 2015 (Figure 3).
Case history
LBP symptoms were not unusual or unexpected for this patient. She has experienced past events of thoracic and lumbar pain due to intensive use of computer, excessive weight lifting and pregnancies. In addition, she reported being an “average” cigarette smoker, doing sedentary work but also being quite diligent about her eating habits (Body Mass Index swaying between 21.6 and 23.6 in the last ten years). She has lived an active life during her free time and she has done “off and on” different sport activities during the last ten years (pilates, swimming, at-home and at the gym fitness workout). Moreover, 33 years earlier when she has been an elite highjumper athlete, she has underwent an open left Achilles tendon repair with longitudinal posteromedial incision, using the Krackow technique. The acute AT total rupture has occured during the straight line running phase in preparation for a highjump attempt. After surgery, she has wore a cast for 12 weeks: Femoral-podalic cast for 4 weeks followed by a short leg cast for 4 weeks (crutches for the first 8 weeks) and fiberglass cast for the latter 4 weeks. Then she has underwent a mild traditional rehabilitation program. As a consequence of the AT rupture event, her body CoP slightly skewed to the left and forward, the left heel has been forced to varus position, the normal spine curvatures has been reduced and the sacrum has been verticalized. These changes in spino-pelvic parameters resulted in a general postural instability in standing and walking. Before February 2021, the Achilles tendon Total Rupture Score (ATRS) [23] was 39%.
Initial neurosurgical Examination Findings: during the examination, the patient showed a positive straight leg raising test (Lasegue sign) at 60° on the left, while the Wassermann’s test was bilaterally negative. Manual testing revealed weakness and mass reduction of the left gastrocnemius muscle and increased AT thickness. Reduced plantar flexors performance has been also detected on the left side. The Lower Extremity Functional [24] and the Oswestry Low Back Pain Disability 2.1a [25] scales scored 15% and 66% respectively.
Interventions and outcome
Surgical Intervention and Management: On the 30th of April 2021, the patient undergone to left L5-S1 microdiscectomy, interlaminar osteophytosectomy and foraminotomy. The surgeon reported a significant amount of epidural pathological tissue around the left root that, once examined, has been classified as a sign of chronic inflammation without atypical elements. The day after the surgical intervention she walked wearing a semi-rigid back brace. Prescription for the 30 days after the surgery included bed resting and incremental walking activity from 30 to 90 minutes per day.
Physiotherapy intervention: One month after the surgical intervention, the patient underwent a physiotherapy assessment for planning a tailored exercise program, aimed to manage pain and to increase mobility, balance and coordination. At the visit, the patient presented with weakness and burning in her left hip and buttock area, weakness and tiredness in the left leg. She also reported pain and limitation in rolling over, getting up from the floor, walking and sitting for more than 10 minutes. Functional Movement Screen (FMS) score was null [26].
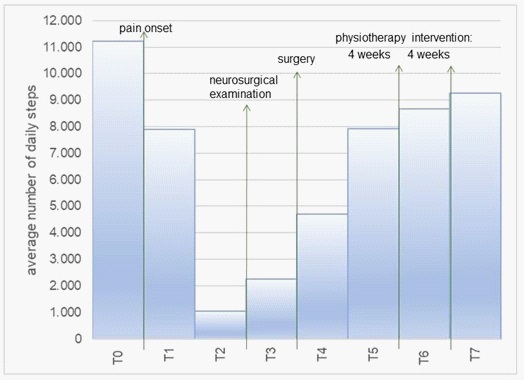
The tailored 8-weeks exercise program included three sessions per week: In each session 90 minutes was dedicated to physical activities on dry land and 40 minutes was dedicated to active and passive aquatic physiotherapy, practiced in a hydrotherapy pool with warm water. Dry land activity included open and closed kinetic chain movements mainly focused on: (a) aerobic training for increasing the V̇o2 max lowered by the bed resting, (b) strengthening the muscles that support the spine and (c) stretching hamstrings. Furthermore, the program included diaphragmatic breathing exercises to improve the core muscle stability. Active hydrotherapy focused on increasing the range of joint movement, strengthening the legs and arms muscles and increasing lumbar curvature. Passive hydrotherapy mainly aimed to stretch and relax the spine muscles. Physical activity rate was quantified using the average number of daily steps, collected trough a wearable accelerometer the patient already wore before the disc herniation event (Figure 4) for 24 hours/day, except for showering and when performing water-based activities (i.e., hydroterapy).
Figure 4 describes the distribution of the average number of daily steps performed during each phase of the patient’s diagnostic and therapeutic pathway. T0: 2 weeks before the first symptoms; T1: from the pain onset to the sudden worsening (1 week); T2: from the worsening to the neurosurgical visit (2 weeks); T3: from the visit to the surgery (4 weeks); T4: postsurgery (4 weeks); T5: physiotherapy intervention (first 4 weeks); T6: physiotherapy intervention (second 4 weeks); T7: 4 weeks after the end of the physiotherapy intervention.
At the fourth week of the program, the patient reported improved capacity in rolling over, getting up from the floor and walking for at least 30 minutes. At the end of the training program the patient gained a good postural recovery. The average numer of daily steps amounted to 77% of the number reported before the disc herniation event (8 662 vs 11 216 steps), not considering the number of steps performed during the physiotherapy sessions (Figure 4). The Lower Extremity Functional Scale [24] and the Oswestry Low Back Pain Disability 2.1a [25] scored 65% and 16% respectively. Furthermore, she got a score of three within the FMS protocol in performing the hurdle step, testing the shoulder mobility, the core stabilization (trunk stability) and the rotary stability. Some compensatory patterns were still put in place during the deep squat, the inline lunge and the active straight-leg raise movements in particular on the left side (FMS score equal to two, bilaterally). These compensatory patterns were perceived by the patient as more correlated to the chronic AT limitations than to the recent back surgery experience. The mild increase of the Achilles tendon Total Rupture Score [23] from 39% to 46% confirmed the patient’s perception.
Insights of the study
Recent studies stated that patients with lumbar degenerative disease were characterized by an anteriorsagittal imbalance, a loss of lumbar lordosis, and an increase of pelvis tilt [27,28]. Moreover, LBP has long been connected to postural and structural asymmetries [29]. Pelvic asymmetry is associated with altered mechanics in the lumbar spine and it has been identified as a good indicator for functional deficit in LBP subjects [30], even though pain seems to be more strictly related to the loss of distribution of load rather than to the loss of stability in the vertebral column [31]. Trunk asymmetry may affect side location of disc herniation and may cause persistent pain after surgery [32]. Despite all medical efforts, evidences reported that individuals with a history of AT rupture have decreased ankle joint proprioception, decreased plantar flexor muscle volume, increased AT length and altered AT stiffness [33-35]. In particular, compared to healthy people, individuals with history of AT rupture show in the affected limb a reduced ankle range of motion during the push-off phase of stance, a reduced knee flexion during the initial contact and an increased knee range of motion during the subsequent phase of weight loading [36]. Furthermore, plantar flexors group is primarily responsible for a braking action with respect to the CoM fall in late stance phase and asymmetric motion of the CoM [37]. In addition, clinical evidences show that longer immobilization times during the AT rupture postoperative phase could increase long-term deficits and foot and ankle compensatory mechanisms onset [38].
In our opinion, the lumbar disc herniation (L5-S1) affected our patient is strictly related to the long-term postural instability led by the AT rupture she has experienced 33 years before and, in particular, by the long time of cast immobilization (12 weeks) and the lack of an early rehabilitation program. Our hypothesis finds an indirect confirmation both in the patient’s perceptions during the recent physiotherapy intervention, the magnitude of the most recent ATRS score and the FMS scores totalized during the deep squat (rounding or arching of the thoracic spine, and asymmetrical weight shifting), the inline lunge (impaired trunk stability and 195 balance) and the active straight-leg raise (limited hamstring and calf flexibility, pelvic and hip mobility) movements. The patient’s treatment pathway (L5-S1 surgery followed by the 8-weeks physiotherapy intervention) showed a good outcome in terms of pain control and mobility increase, but the existing compensatory patterns for balancing the pelvic asymmetry, associated to the postural instability, need of being further corrected. A further tailored training program should be identified to make the distribution of load more efficient along the spine, also considering the degenerative conditions affecting the cervical and thoracic levels. In particular the program should follow the Global Postural Reeducation (GPR) method to improve postural symmetry by treating the patient with specific static postures exploiting eccentric orisometric muscle contractions with increasing length [39]. GPR considers the existence of a series of interconnected muscles playing specific functional roles, e.g the posterior static chain and the anterior diaphragmatic chain. GPR method promotes postural symmetry by stretching the shortened muscle chains and enhancing the contraction of the antagonists [39]. Furthermore, the GPR strategy is based on three principles: (1) individuality (each person is a unique), (2) causality (the true cause of a musculoskeletal condition may arise from distant sites), and (3) totality (the body should be treated in its entirety) [39].
The tailored program should also be integrated by hydrotherapy sessions for promoting cardiovascular fitness, functional strengthening exercises and gait normalisation activities, while reducing the high loads that running and jumping on land produces in the tendon [40].
Conclusion
This case study highlights the biomechanical role of the posterior kinetic chain in maintaining the spine healthy and it shows how the effect of long-term compensatory mechanisms increase the risk of lumbar degenerative diseases onset. Addictionally, it points out how the lack of an early functional rehabilitation protocol for the AT rupture can impact the efficiency of spine injury treatment in the future. Finally, trough the description of this case the authors hope to improve the awareness of health care professionals about the need of: (1) perfoming cohmprensive and multidisciplinary evalutaion of the body in its entirety, by considering all the current and past neuromusculoskeletal dysfunctions, (2) promoting tailored programmes of physical activity built on the individual profile of each patient and (3) combining activities on dry land and hydrotherapy within the same physical session, to improve the efficacy of rehabilitation programmes for spine injuries.
Declarations
Ethical approval: Not applicable
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors.
Conflict of interest: None.
Acknowledgements: The authors thank the staff of the San Rossore Sport Village and MSc Stefania Pieroni for having supported in the preparation of the electronic illustrations.
Autorship: Conception and design of the study: Michela Franchini; acquisition of data: Michela Franchini, Jacopo Giorgetti, Alessia Formica, Simone Casarosa; interpretation of data: Michela Franchini, Jacopo Giorgetti; Simone Casarosa, drafting the article: Michela Franchini; revising it critically for important intellectual content: Jacopo Giorgetti; Alessia Formica, Simone Casarosa; final approval of the version to be submitted: Michela Franchini, Jacopo Giorgetti, Alessia Formica, Simone Casarosa.
References
- Huang YP, Bruijn SM, Lin JH, Meijer OG, et al. Gait adaptationsin low back pain patients with lumbar disc herniation: Trunk coordination and arm swing. Eur Spine J. 2011; 20: 491-499.
- Yang H, Liu H, Li Z, et al. Low back pain associated with lumbar disc herniation: Role of moderately degenerative disc and annulus fibrous tears. Int J Clin Exp Med. 2015; 8: 1634-1644.
- Bento TPF, Genebra CVDS, Maciel NM, Cornelio GP, Simeão SFAP, et al. Low back pain and some associated factors: Is there any difference between genders? Braz J Phys Ther. 2020; 24: 79-87.
- Azfar SM, Murad MA, Azim SR, Baig M. Frequency of and Various Factors Associated with Stress, Anxiety, and Depression among Low Back Pain Patients. Cureus. 2019; 11: e5701.
- Demoulin C, Crielaard JM, Vanderthommen M. Spinal muscle evaluation in healthy individuals and low back-pain patients: A literature review. Joint Bone Spine. 2007; 74: 9-13.
- Gwilym SE, Oag HC, Tracey I, Carr AJ. Evidence that central sensitisation is present in patients with shoulder impingement syndrome and influences the outcome after surgery. J Bone Joint Surg Br. 2011; 93: 498-502.
- O’Neill S, Manniche C, Graven-Nielsen T, Arendt-Nielsen L. Generalized deep-tissue hyperalgesia in patients with chronic low-back pain. Eur J Pain. 2007; 11: 415-420.
- Tompra N, van Dieën JH, Coppieters MW. Central pain processing is altered in people with Achilles tendinopathy. Br J Sports Med. 2016; 50: 1004-1007.
- Plinsinga ML, van Wilgen CP, Brink MS, Vuvan V, Stephenson A, et al. Patellar and Achilles tendinopathies are predominantly peripheral pain states: A blinded case control study of somatosensory and psychological profiles. Br J Sports Med. 2018; 52: 284-291.
- Betsch M, Schneppendahl J, Dor L, Jungbluth P, Grassmann JP, et al. Influence of foot positions on the spine and pelvis. Arthritis Care Res (Hoboken). 2011; 632: 1758- 1765.
- Menz HB, Dufour AB, Riskowski JL, Hillstrom HJ, Hannan MT, et al. Foot posture, foot function and low back pain: the Framingham Foot Study. Rheumatology (Oxford). 2013; 52: 2275-2282.
- . Hamel AJ, Sharkey NA, Buczek FL, Michelson J. Relative motions of the tibia, talus, and calcaneus during the stance phase of gait: a cadaver study. Gait Posture. 2004; 20: 147-153.
- Pedowitz D, Kirwan G. Achilles tendon ruptures. Curr Rev Musculoskelet Med. 2013; 6: 285-293.
- Jandacka D, Zahradnik D, Foldyna K, Hamill J. Running biomechanics in a long-term monitored recreational athlete with a history of Achilles tendon rupture. BMJ Case Rep. 2013: bcr2012007370.
- Proske U. Kinesthesia: The role of muscle receptors. Muscle Nerve. 2006; 34: 545-558.
- Fugl-Meyer AR, Nordin G, Sjöström M, Wählby L. Achilles tendon injury. A model of isokinetic strength training using biofeedback. Scand J Rehabil Med. 1979; 11: 37-44.
- Garrett WE Jr, Califf JC, Bassett FH 3rd. Histochemical correlates of hamstring injuries. Am J Sports Med. 1984; 12: 98-103.
- Olsson N, Nilsson-Helander K, Karlsson J, Eriksson BI, Thomée R, et al. Major functional deficits persist 2 years after acute Achilles tendon rupture. Knee Surg Sports Traumatol Arthrosc. 2011; 19: 1385-1393.
- Willits K, Amendola A, Bryant D, Mohtadi NG, Giffin JR, Fowler P, Kean CO, Kirkley A. Operative versus nonoperative treatment of acute Achilles tendon ruptures: A multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg Am. 2010; 92: 2767-2775.
- Khan RJ, Fick D, Brammar TJ, Crawford J, Parker MJ, et al. Interventions for treating acute Achilles tendon ruptures. Cochrane Database Syst Rev. 2004; CD003674.
- Powell HC, Silbernagel KG, Brorsson A, Tranberg R, Willy RW, et al. Individuals Post Achilles Tendon Rupture Exhibit Asymmetrical Knee and Ankle Kinetics and Loading Rates During a Drop Countermovement Jump. J Orthop Sports Phys Ther. 2018; 48: 34-43.
- Woodard CM, James MK, Messier SP. Computational methods used in the determination of loading rate: Experimental and clinical implications. J Appl Biomech. 1999; 15: 404-417.
- Nilsson-Helander K, Thomeé R, Silbernagel KG, Thomeé P, Faxén E, Eriksson BI, Karlsson J. The Achilles tendon Total Rupture Score (ATRS): Development and validation. Am J Sports Med. 2007; 35: 421-426. Erratum in: Am J Sports Med. 2011; 39: NP8. GrävareSilbernagel, Karin [corrected to Silbernagel, Karin Grävare].
- Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): scale 301 development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999; 79: 371-383.
- Monticone M, Baiardi P, Ferrari S, Foti C, Mugnai R, et al. Development of the Italian version of the Oswestry Disability Index (ODI-I): A cross-cultural adaptation, reliability, and validity study. Spine (Phila Pa 1976). 2009; 34: 2090-2095.
- Minick KI, Kiesel KB, Burton L, Taylor A, Plisky P, et al. Interrater reliability of the functional movement screen. J Strength Cond Res. 2010; 24: 479-486.
- Barrey C, Roussouly P, Perrin G, Le Huec JC. Sagittal balance disorders in severe degenerative spine. Can we identify the compensatory mechanisms? Eur Spine J. 2011; 20 Suppl 5: 626- 633.
- Barrey C, Jund J, Noseda O, Roussouly P. Sagittal balance of the pelvis-spine complex and lumbar degenerative diseases. A comparative study about cases. Eur Spine J. 2007; 16: 1459-1467.
- Al-Eisa E, Egan D, Deluzio K, Wassersug R. Effects of pelvic asymmetry and low back pain on trunk kinematics during sitting: A comparison with standing. Spine (Phila Pa 1976). 2006; 31: E135- E143.
- Al-Eisa E, Egan D, Deluzio K, Wassersug R. Effects of pelvic skeletal asymmetry on trunk movement: Three-dimensional analysis in healthy individuals versus patients with mechanical low back pain. Spine (Phila 319 Pa 1976). 2006; 31: E71-E79.
- Kasim E, Er U, Simsek S, Kazanci A, Guclu B, et al. Does short segment lumbar stabilization and fusion accelerate adjacent uppersegment instability? J Turk Spinal Surg. 2013; 24: 117-122.
- Kanat A, Yazar U, Ozdemir B, Kazdal H, Balik MS, et al. Neglected knowledge: Asymmetric features of lumbar disc disease. Asian J Neurosurg. 2017; 12: 199-202.
- Bressel E, Larsen BT, McNair PJ, Cronin J. Ankle joint proprioception and passive mechanical properties of the calf muscles after an Achilles tendon rupture: A comparison with matched controls. Clin Biomech (Bristol, Avon). 2004; 19: 284-291.
- Rosso C, Vavken P, Polzer C, Buckland DM, Studler U, et al. Longterm outcomes of muscle volume and Achilles tendon length after Achilles tendon ruptures. Knee Surg Sports Traumatol Arthrosc. 2013; 21: 1369-1377.
- Agres AN, Duda GN, Gehlen TJ, Arampatzis A, Taylor WR, et al. Increased unilateral tendon stiffness and its effect on gait 2-6 years after Achilles tendon rupture. Scand J Med Sci Sports. 2015; 25: 860- 867.
- Jandacka D, Silvernail JF, Uchytil J, Zahradnik D, Farana R, et al. Do athletes alter their running mechanics after an Achilles tendon rupture? J Foot Ankle Res. 2017; 10: 53.
- Tesio L, Rota V. The Motion of Body Center of Mass During Walking: A Review Oriented to Clinical Applications. Front Neurol. 2019; 10: 999.
- Xu, XY, Gao S, Lv Y. et al. Duration of immobilisation after Achilles tendon rupture repair by open surgery: A retrospective cohort study. J Orthop Surg Res. 2021; 16.
- Ferreira GE, Barreto RG, Robinson CC, Plentz RD, Silva MF, et al. Global Postural Reeducation for patients with musculoskeletal conditions: A systematic review of randomized controlled trials. Braz J Phys Ther. 2016; 20: 194-205.
- Beneka AG, Malliou PC, Benekas G. Water and land based rehabilitation for Achilles tendinopathy in an elite female runner. Br J Sports Med. 2003; 37: 535-537.