
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Voriconazole induced periostitis
Priya Reddy*; Manisha Kumar
Scripps Clinic/Green Rheumatology, San Diego, California, USA.
*Corresponding Author: Priya Reddy
Scripps Clinic/Green Rheumatology, San Diego,
California, USA.
Email: pred81993@gmail.com
Received : Jan 08, 2022
Accepted : Feb 11, 2022
Published : Feb 18, 2022
Archived : www.jcimcr.org
Copyright : © Reddy P (2022).
Citation: Reddy P, Kumar M. Voriconazole induced periostitis. J Clin Images Med Case Rep. 2022; 3(2): 1674.
Description
Voriconazole is a second generation broad spectrum triazole antifungal agent which is commonly used for prophylaxis and treatment of invasive aspergillosis, especially in patients with solid organ and hematopoietic stem cell transplants. One of the rare, adverse effects of long-term use is periostitis which is caused by increased circulating levels of fluoride from voriconazole metabolism with clinical findings similar to skeletal fluorosis. Given the increased use of voriconazole, it is essential to recognize periostitis as an adverse effect with prompt discontinuation of the medication improving patient outcomes and quality of life.
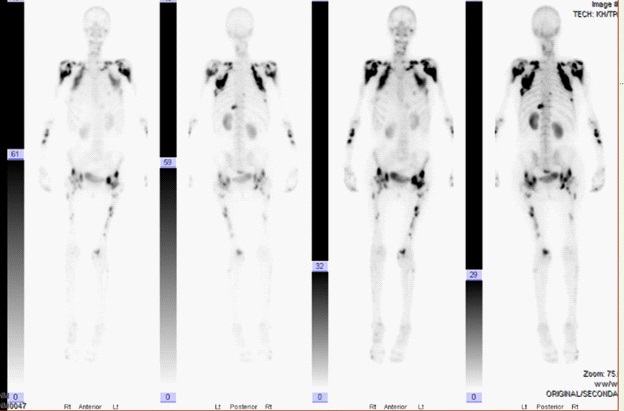
A 73-year old Caucasian female with history of coccidioidalmycosis meningitis status post ventriculoperitoneal shunt on suppressive voriconazole presented to rheumatology clinic with progressive decline characterized by diffuse bony pain and arthralgias. The pain started six months following initiation of voriconazole with symptoms unresponsive to acetaminophen, ibuprofen, pregabalin and physical therapy. Physical examination revealed a thin wheelchair bound female with diffuse bony tenderness and hand muscle wasting. Laboratory work-up was notable for elevated alkaline phosphatase 739 U/L (reference value 38-126 U/L), alkaline phosphatase- bone 480 U/L (reference value 0-55 U/L), gamma-glutamyl transferase 324 U/L (reference value 5-55 U/L), C-reactive protein 7.8 mg/L (reference range <10 mg/L) and erythrocyte sedimentation rate 86 mm/hour (reference value <30 mm/hr). Autoimmune work-up and thyroid studies were unremarkable. Technetium-99 m bone scan demonstrated markedly abnormal osseous uptake along the scapular margins, proximal shafts of both humeri and bilateral hips with additional focal abnormalities in bilateral forearms, femoral shafts and proximal left eleventh rib (Figure 1). These findings favored periostitis likely related to long term voriconazole treatment. Patient was subsequently transitioned off voriconazole to itraconazole with complete resolution of her bony pain after one month.
References
- Guarascio AJ, Bhanot N, Min Z. Voriconazole-associated periostitis: Pathophysiology, risk factors, clinical manifestations, diagnosis, and management. World J Transplant. 2021; 11: 356-371.
- Rad B, Saleem M, Grant S, Florkowski C, Coates P, Gordon D, Rankin W, et al. Fluorosis and periostitis deformans as complications of prolonged voriconazole treatment. Ann Clin Biochem. 2015; 52: 611-614.
- Skaug M, Spak C, Oza U. Painful periostitis in the setting of chronic voriconazole therapy. Proceedings (Baylor University. Medical Center). 2014; 27: 350–352. https://doi.org/10.1080/0 8998280.2014.11929156.