
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Laparoscopic surgery for adrenal ganglioneuroma: Case report and literature review
Wendel Souza Kruschewsky1*; Felipe Gonçalves Moreira2; Diogo Lago Morbeck3; Leonardo Marques Calazans1; Nilo Jorge Carvalho Leão Barretto1; Ewerton Pedrosa Muragaki1; Lais Fernandes4; Filipe Catarino5
1 Preceptor of Urology at Hospital Santo Antônio, Avenida Dendezeiros do Bonfim, Brazil.
2 Urology Resident, Hospital Santo Antônio, Avenida Dendezeiros do Bonfim, Brazil.
3 Pathologist at Hospital Santo Antônio, Avenida Dendezeiros do Bonfim, Brazil.
4 Medicine Student, UNIFTC, Avenida Luís Viana Filho, 8812, Paralela. Salvador/Bahia, Brazil.
5 Medicine Student, UFBA Av Reitor Miguel Calmon, s/n, Vale do Canela - CEP: 40110-906 | Salvador, Brazil.
*Corresponding Author: Kruschewsky WS
Preceptor of Urology at Hospital Santo Antônio,
Avenida Dendezeiros do Bonfim, 161, Salvador-BA,
40301-155, Brazil.
Email: wendel.krus@gmail.com
Received : Jan 18, 2022
Accepted : Feb 14, 2022
Published : Feb 21, 2022
Archived : www.jcimcr.org
Copyright : © Kruschewsky WS (2022).
Keywords: adrenal ganglioneuroma; laparoscopy; adrenal tumor.
Citation: Kruschewsky WS, Moreira FG, Morbeck DL, Calazans LM, Barretto NC, et al. Laparoscopic surgery for adrenal ganglioneuroma: Case report and literature review. J Clin Images Med Case Rep. 2022; 3(2): 1679.
Introduction
Ganglioneuromas (GN) are benign and well-differentiated tumors originated from the sympathetic chain of the neural crest. They can affect any part of the body along the autonomic ganglia, however the two most common sites of presentation are in the retroperitoneal space (32-52%) and posterior mediastinum (39-43%), followed by the cervical region (8-9%) [6]. They are most common in children and young adults, but can occur at any age. They have a greater predilection for females (3:1). They are usually asymptomatic and when present, clinical manifestations are symptoms of compression (epigastric pain, abdominal pain). Most adrenal ganglioneuromas do not have endocrine production, but up to 30% of tumors can secrete testosterone or catecholamines.
Case report
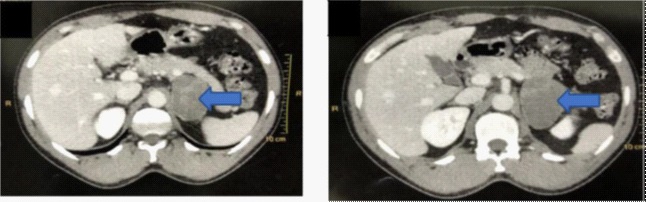
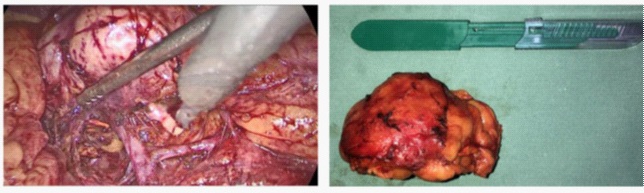
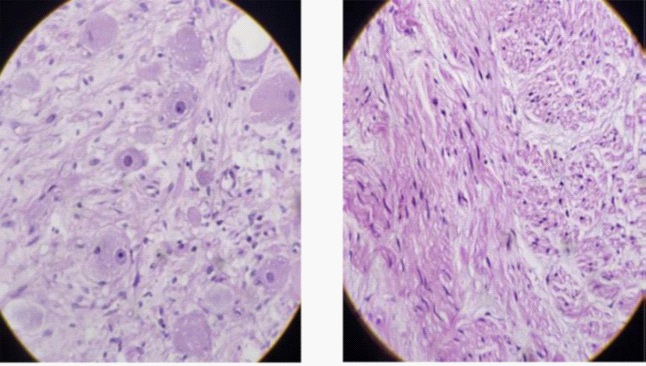
Male patient, 39 years old, without comorbidities, referred to Hospital Santo Antônio – Obras Sociais Irmã Dulce due to a nodular image shown in routine exams. The patient was asymptomatic in a specialized medical appointment. Abdominal ultrasonography showed an expansive formation in the topography of the left adrenal, measuring 5.5 cm in the longest axis. A computed tomography scan of the abdomen showed solid expansive formation and heterogeneous post-contrast highlight in the left adrenal, with médium density of 26 UH and measuring about 6.2 X 5.8 cm in its longest axes (Figures 1 and 2). In requested metabolic assessment, all results were unchanged. The patient underwent videolaparoscopic left adrenalectomy (Figures 3 and 4). The patient evolved without complications and was discharged on the first postoperative day. Pathological anatomy results revealed a mature subtype of ganglioneuroma, with ganglion cell and Schwann cell components (Figures 5 and 6). Size of neoplasm: 8.0 X 5.5 X 4.0 cm. Neoplastic components: ganglion cells and Schwann cells. Characteristics of the ganglionic component: mature with compact and eosinophilic cytoplasm with distinct cell borders, single eccentric nucleus, prominent nucleolus, varying in distribution and number, with sparse distribution. Characteristic of the Schwann cell component: they support neuritic processes without the presence of myxoid component.
Discussion
Adrenal ganglioneuroma is a rare, nonfunctioning, benign tumor of the adrenal gland that develops slowly. Although in rare cases there is metabolic production of testosterone and catecholamine, the vast majority presents as an adrenal incdentaloma on imaging exams [7]. Symptoms are only present if the tumor is large enough to cause a mass effect on adjacent structures or if it exhibits hormonal activity [4]. The test used to confirm the existence of adrenal incidentaloma is abdominal CT scan. Adrenal incidentalomas are rare findings on abdominal CT (0.6 to 1.3% of all abdominal CT scans performed). Adrenal ganglioneuroma represents only 0-6% of all adrenal incidentalomas [7].
Differential diagnosis includes: ganglioneuroblastoma, neuroblastoma, pheochromocytoma, adrenal adenoma, and adrenal carcinoma [6]. Diagnostic confirmation requires histopathological analysis which reveals a neoplasm formed by a mixture of ganglion cells and Schwann cells. Ganglion cells may exhibit a mature to slightly dysmorphic component. The mature component exhibits eosinophilic compact cytoplasm cells with distinct cell borders, single eccentric nucleus, and prominent nucleolus. And the dysmorphic component presents cells with single or multiple pyknotic nuclei, varying in distribution and number, which are usually quite sparse. May contain finely grained, golden to brown pigment (lipofuscin or neuromelanin). The Schwann cell component may involve neuritic processes and get organized into small, intersecting fascicles that are separated by a loose myxoid stroma. Ganglioneuroma has two histological subtypes: mature (most common, where all ganglion cells are mature) and maturing (where there is a smaller component of scattered collections of differentiating neuroblasts or maturing ganglion cells). However, unlike the mixed ganglioneuroblastoma subtype, these immature focuses do not form clear microscopic nests. A slight variation in cellularity is allowed for these diagnoses, however, no significant atypia, mitosis or necrosis should be present. Most cases are of sporadic origin, but some rare cases have been reported in association with Turner Syndrome and Multiple Endocrine Neoplasia Type II [2].
The definitive treatment for adrenal ganglioneuroma is surgical resection, open or minimally invasive (laparoscopic, robotic). Adrenal tumor larger than 6 cm is a relative contraindication for a laparoscopic approach [8]. It should only be performed in tumors larger than 6 cm by an experienced team and respecting all the oncological principles of resection. In our case, despite the tumor being larger than 6 cm, the laparoscopic approach was chosen, without violating the surgical principles of adrenal surgery, and without intraoperative complications.
Conclusion
Adrenal ganglioneuroma is a rare tumor, usually benign, composed of mature ganglion cells and Schwann cells. It usually does not cause symptoms until it reaches a sufficient volume to cause compressive symptoms. In most cases the diagnosis is through an incidentaloma in imaging exams. We report the case of a 39-year-old young patient with an incidental finding of a left adrenal lesion measuring 6.2 cm in the longest axis, who underwent videolaparoscopic adrenalectomy without complications. The prognosis tends to be excellent in these cases, with no recurrence or need for adjuvant therapy
References
- Leavitt JR, Harold DL, Robinson RB. Adrenal ganglioneuroma: a familial case. Urology. 2000; 56(3): 508. doi: 10.1016/s0090- 4295(00)00695-6. PMID: 10962331.
- Burroughs M A, Urits I, Viswanath O, et al. Adrenal Ganglioneuroma: A Rare Tumor of the Autonomic Nervous System. Cureus. 2020; 12(12): e12398. DOI 10.7759/cureus.12398
- Yu Y, Zeshen W, Jiahao Z, Hongwei W, Bentao S. Adrenal Ganglioneuroma: A Rare Case Report and Literature Review. Urol Nephrol Open Access. 2017; J 5(5): 00185. DOI: 10.15406/unoaj.2017.05.00185
- Oliveira AF, TCBC-MG, José L, Vieira, Moreira AA, ACBC-MG , et al. Ganglioneuroma retroperitoneal. Relato de caso. Relatos Casos Cir. 2015; (1): 1-3.
- Mylonas KS, Schizas D, Economopoulos KP. Adrenal ganglioneuroma: What you need to know. World J Clin Cases 2017; 5(10): 373-377 Available from: URL: http://www.wjgnet.com/2307- 8960/full/v5/i10/373.htm DOI: http://dx.doi.org/10.12998/ wjcc.v5.i10.373
- Estrela JRSS, Ziomkowski AA, Mascarenhas F, Matos AC. A Rare Case of an Adrenal Ganglioneuroma Treated Laparoscopically in a Patient with Left-Sided Inferior Vena Cava. J Endourol Case Rep. 2020; 29; 6(4): 530-532. doi: 10.1089/cren.2020.0174. PMID: 33457721; PMCID: PMC7803268.
- Sapalidis K, Mandalovas S, Kesisoglou I. Laparoscopic Excision of an Adrenal Ganglioneuroma Presented as an Incindentaloma of the Retro Peritoneum. Curr Health Sci J. 2018; 44(1): 71-75. doi:10.12865/CHSJ.44.01.12.
- Campbell-Walsh Urology, 11ª edição, 4 volumes, Caplan, Louis R; Wein, Alan J; Peters, Craig; Kavoussi, Louis R.