
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Simultaneous vestibular, orbital, meningeal and medullary involvement in a patient diagnosed with neurofibromatosis type 2
Ndayishimiye V*; Hasnaa B; Achta AF; Bamba A; Merzem A; Amriss O; Moussali N; El Benna N
Department of Radiology, 1953 Hospital, Ibn Rochd University Hospital Center of Casablanca, Morocco, Hassan II University of Casablanca, Moroccco.
*Corresponding Author: Vianney Ndayishimiye
Department of Radiology, Radiology Service of
August 20, 1953 Hospital, Ibn Rochd University
Hospital Center of Casablanca, Morocco, Hassan II
University of Casablanca, Moroccco.
Email: vianneybienvenu@gmail.com
Received : Dec 30, 2021
Accepted : Feb 15, 2022
Published : Feb 22, 2022
Archived : www.jcimcr.org
Copyright : © Ndayishimiye V (2022).
Abstract
Neurofibromatosis Type 2 (NF2) is an autosomal dominant genetic disease characterized by the presence of bilateral vestibular schwannomas. We report the case of a 21-year-old patient, followed up for neurofibromatosis type 2, operated two times for right parietal and orbital meningioma that complained for headache and dizziness, referred to us for brain and cervical MRI exploration including 3D-FIESTA sequence. MRI completed by CT scan noted intraosseous and cerebral extra-axial meningiomas, bilatetal shwannomas and cervical epedymomas. Neurofibromatosis type 2 is a genetic disease with nervous system lesions and MRI is important for their exploration.
Keywords: neurofibromatose type 2; schwannomas; meningiomas; ependymomas.
Citation: Ndayishimiye V, Hasnaa B, Achta AF, Bamba A, Merzem A, et al. Simultaneous vestibular, orbital, meningeal and medullary involvement in a patient diagnosed with neurofibromatosis type 2. J Clin Images Med Case Rep. 2022; 3(2): 1685.
Introduction
Neurofibromatosis Type 2 (NF2) is a phacomatosis involving developmental abnormalities of ectodermal tissue, and leading to the formation of cutaneous, nerve and ocular “phacomas”. It is an autosomal dominant genetic disorder with high penetrance, linked to the mutation of the NF2 gene on chromosome 22 encoding schwannomine. The goal of our work is to describe in Magnetic Resonance Imaging (MRI) the neurological lesions encountered in a patient with neurofibromatosis type 2.
Case presentation
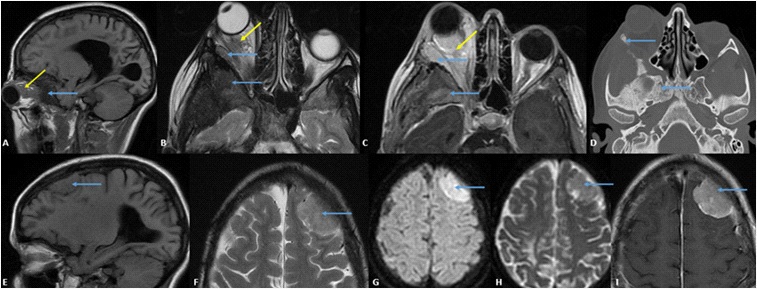
We report the case of a 21-year-old patient, followed up for neurofibromatosis type 2, operated respectively in 2015 and 2018 for right parietal and orbital meningioma, who had complained for 3 years of headache and dizziness with grade 3 right exophthalmos referred to us for MRI brain exploration. MRI with injection of contrast product with a protocol including the 3D-FIESTA sequences on the pontocerebellar angles was carried out and noted a tissue process centered on the sphenoid large wing and the outer wall of the right orbit in T1 hypointense, T2 heterogeneous hypersignal, heterogeneously enhanced after injection of Gadolinium. It measured 8 X 5 X 4 cm. Further to the CT scan, we noted irregular thickening of the sphenoid bone, the right temporal bone and the right orbital bones, related to intraosseous meningiomas.
There was associated a meningeal thickening opposite and extension in intraorbital, realizing a tissue mass of 4 X 2 cm, extended over 2 cm, responsible for an encompassment of the external rectus muscle, filling of intra and extraconic fat, repression of the superior rectus muscle and the optic nerve responsible for grade 3 exophthalmos.
We also noted two left oval frontal extra-axial formations, with a large meningeal implantation base, meningeal thickening opposite, in T1 isosignal, discrete T2 heterogeneous hypersignal, diffusion hypersignal with an intermediate ADC measuring 36 X 21 mm, extended over 28 mm for the most voluminous, related to cerebral meningiomas (Figure 1).
We noted also bilateral formations of the pontocerebellar angles in icecone, in T1 hyposignal, T2 hypersignal and diffusion heterogeneous hypersignal with an intermediate ADC measuring 23 X 16 mm on the right and 23 X 23 mm on the left (green arrows), widening the internal auditory canal. These formations are intensely enhanced after injection of gadolinium, compatible with bilateral vestibular schwannomas. On cervical sections, we noted two intramedullary formations at the level of C3 and D1, heterogeneously enhanced after injection of gadolinium measuring 23 X 9 mm and 7 mm respectively, compatible with ependymomas (Figure 2).

Discussion
Neurofibromatosis type 2 (NF2) is an autosomal dominant genetic disease characterized by the presence of bilateral vestibular schwannomas, formerly known as acousticneuromas. It is a rare and potentially severe disease, responsible for a marked decrease in the autonomy and life expectancy of patients. It is most often diagnosed in young adults, but can occur at any age of life. The manifestations of NF2 are not limited to vestibular schwannomas, other benign tumors; meningiomas, schwannomas and ependymomas; are also encountered, associated with cutaneous and ophthalmological manifestations [1]. Large population-based analyzes have suggested that genetic mutations in NF2 are present in approximately 1 in 25,000 people with no gender predilection [2].
The mode of appearance of vestibular schwannomas is the on set of sensorineural hearing loss usually between the ages of 18 and 24, sometimes in childhood, but never after age 30. Schwannomas can affect the cranial nerves and spinal cord Meningiomas, astrocytomas or associated ependymomas have a poor prognosis. Associated dermatological signs are rarer. These are ‘café-au-lait’ spots and some skin or subcutaneous neurofibromas. Ocular signs are often associated, due to posterior subcapsular or capsular cataract (from an early age), as well as gliomas of the papilla and epiretinal membranes. A meningioma of the optic nerve can complicate the situation [3].
Various tumors of the spine can occur in patients with NF2 and can be found in the cervical, thoracic and lumbar region. These tumors are further classified as extramedullary or intramedullary tumors based on their presentation relative to the spinal cord. Extramedullary tumors are usually schwannomas or meningiomas, while intramedullary tumors are often ependymomas, but they can be astrocytomas or schwannomas [4]. Meningiomas are the second tumor found in individuals with NF2. Intracranial meningiomas are seen in 45% to 58%, while spinal meningiomas are found in about 20% of those affected. Intracranial meningiomas tend to be multiple in number and often develop at a younger age than their sporadic counter parts. Meningiomas enhance homogeneously after injection of contrast medium and are best assessed with injected T1-weighted MRI.
Ependymomas are present in 33% to 53% of individuals with NF2, with the cervical cord or cervico-medullary junction being the most frequent an atomical sites of involvement. On MRI, these tumors appear as hyperintense masses on T2-weighted sequences, which are hypointense to isointense on T1-weighted sequences. The majority of ependymomas associated with NF2 are tumors enhanced by contrast product [5]. All patients with suspected NF2 should undergo an MRI scan performed with thin sections through the Internal Auditory Canal (IAC). All patients diagnosed with unilateral vestibular schwannoma should have a series of IAC exams to make sure there is no tumor on the opposite side. Patients diagnosed with NF2 should under go a complete series of spinal MRI scans to assess the spine and stage the disease [6]. Bilateral vestibular schwannoma reveals NF2 in 50% of cases. MRI in T1 before and after injection of gadolinium and in T2 3D sequence of the CISS or FIESTA type is effective in demonstrating bilateral vestibular schwannoma. These tumors appear hyperintense in proton density, T2 and FLAIR. Areas of necrosis and cysts are rare. Neuromas are often asymmetric. Uni or bilateral schwannomas can be noted in all cranial nerves from III to XII [7].
Conclusion
Neurofibromatosis type 2 is a familial tumor predisposition syndrome characterized by the development of distinctive lesions of the nervous system, including bilateral vestibular schwannomas, multiple spinal and peripheral schwannomas, meningiomas and ependymomas, MRI is the examination modality of choice for exploration of the seen countered anomalies.
Declarations
Competing interests: The authors declare no conflict of interest.
Contributions from authors: All the authors contributed to the conduct of this work. They also state that they have read and approved the final version of the manuscript.
References
- Goutagny S, Bouccara D, Bozorg-Grayeli A, Sterkers O, Kalamarides M. Neurofibromatose de type 2. EMC - Neurologie. 2009; 6: 1-11. https://doi.org/10.1016/S0246-0378(09)46751-4.
- Coy S, Rashid R, Stemmer-Rachamimov A, Santagata S. An update on the CNS manifestations of neurofibromatosis type 2. Acta Neuropathol. 2020; 139: 643-665. https://doi.org/10.1007/ s00401-019-02029-5.
- Dubrulle F, Martin-Duverneuil N, Moulin G. Imagerie en ORL. 2010.
- Slattery WH. Neurofibromatosis Type 2. Otolaryngologic Clinics of North America. 2015; 48: 443-460. https://doi.org/10.1016/j. otc.2015.02.005.
- Campian J, Gutmann DH. CNS Tumors in Neurofibromatosis. JCO. 2017; 35: 2378-2385. https://doi.org/10.1200/ JCO.2016.71.7199.
- Hoa M, Slattery WH. Neurofibromatosis 2. Otolaryngologic Clinics of North America. 2012; 45: 315-332. https://doi. org/10.1016/j.otc.2011.12.005.
- Dietemann J-L. Neuro-imagerie diagnostique. Issy-Les-Moulineaux: Elsevier Masson. 2012.