
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Persistent torticollis revealing Sprengel syndrome: A case report and literature review
Ndayishimiye V*; Salihou A; Diarra D; Laoudiyi D; Chbani K; Salam S; Ouzidane L
Pediatric Radiology Service, Abderrahim Harouchi Children’s Hospital, Ibn Rochd Univesrity Hospital Center of Casablanca, Hassan II University of Casablanca, Morocco.
*Corresponding Author: Ndayishimiye Vianney
Pediatric Radiology Service, Abderrahim Harouchi
Children’s Hospital, Ibn Rochd Univesrity Hospital
Center of Casablanca, Hassan II University of Casablanca, Morocco.
Email: vianneybienvenu@gmail.com
Received : Dec 30, 2021
Accepted : Feb 16, 2022
Published : Feb 23, 2022
Archived : www.jcimcr.org
Copyright : © Ndayishimiye V (2022).
Abstract
Sprengel’s deformity is a rare condition, due to the congenital failure of the descent of the scapula. We report the case of an eleven (11) year old patient presenting a permanent flexion attitude of the cervical spine with posterior thoracic swelling in the inner edge of the left scapula and shoulder asymmetry, evolving from early childhood. The limitation of the left shoulder movements and aesthetic discomfort motivated the consultation in the pediatric orthopedics service, which referred her to us for CT scan and MRI imaging exploration. The CT scan noted a seventh thoracic vertebra (C7) posterior arch hypertrophy, of which cortical is in continuity with a costiform bony outgrowth articulating with the superioro-internal angle of the left scapula which is elongated, corresponding to an omovertebral bone. It also noted a vertebral block from C5 to D2 with defective closure of the posterior arches of C2, C5 to C7 and D3 to D5 and a costal bifidity of the transverse process of D1, without anomaly of the spinal cord to the MRI.
Springel’s deformity can be suspected on antenatal ultrasound in the presence of asymmetric thickening of the nuchal soft tissues. In postnatal period, a radiological assessment including the standard radiography and especially the CT scan with its multiplanar reconstructions and the possibility that the MRI to analyze the paravertebral soft tissues and the spinal cord, draw up the diagnosis and analysize of the associated anomalies.
Keywords: deformity; sprengel; congenital; CT scan; MRI.
Citation: Ndayishimiye V, Salihou A, Diarra D, Laoudiyi D, Chbani K, et al. Persistent torticollis revealing Sprengel syndrome. A case report and literature review. J Clin Images Med Case Rep. 2022; 3(2): 1688.
Introduction
Sprengel’s deformity is a rare and complex congenital deformity of the shoulder girdle. The deformity usually occurs sporadically, although in combination with other birth defects, such as congenital scoliosis, fusion of the cervical vertebrae and other situations like Klippel-Feil syndrome can coexist. The goal of our work is to report a new case of symptomatic Sprengel syndrome in children on sectional imaging.
Case presentation
We report the case of an eleven (11) years old patient presenting a permanent flexion attitude of the cervical spine with posterior thoracic swelling in the inner edge of the left scapula and shoulder asymmetry, evolving from early childhood but niglected by the parents. The limitation of the left shoulder movements and aesthetic discomfort motivated the consultation in the pediatric orthopedics service, which referred her to us for CT scan and MRI imaging exploration.
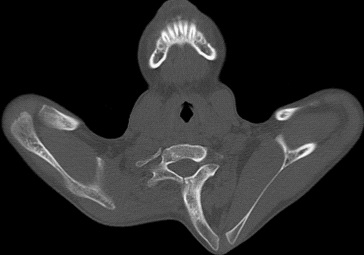
The cervical CT scan without injection of contrast product with multiplanar reconstructions noted on the bone window a straightness of the cervical spine, a seventh thoracic vertebra (C7) posterior arch hypertrophy, of which cortical is in continuity with a costiform bony outgrowth articulating with the superioro-internal angle of the left scapula which is elongated, corresponding to an omovertebral bone (Figure 1). It also noted a vertebral block from C5 to D2 (Figure 2) with defective closure of the posterior arches of C2, C5 to C7 and D3 to D5 and a costal bifidity of the transverse process of D1.

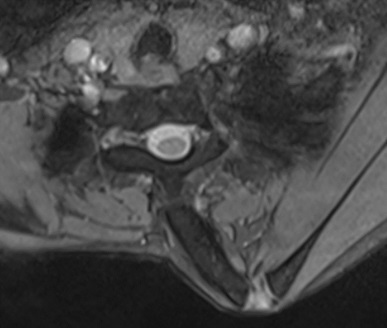
These results motivated the performing of cervical MRI with T2 sagittal and axial and T1 sagittal sequences to analyze the spinal cord and its environment. The omovertebral bone was identified as on a CT scan and there was no bone marrow abnormality (Figure 3).
Discussion
Sprengel’s deformity, also called Sprengel’s anomaly, Sprengel’s shoulder or congenital high scapula is the congenital failure of the descent of the scapula. Eulenburg first described it in 1863. Sprengel described 4 cases in 1891; therefore, the anomaly was called the Sprengel deformation [1]. The pathophysiogenesis of this condition remains unknown. The scapula appears at the 5th week of embryonic life as a mesenchymal mass located opposite C4-C5. It gradually migrates from the 6th to the 12th week to its final physiological position in the caudal direction while also under going external rotation. By the 8th week, its upper edgeis at the level of C7 and its lower angle opposite the 6th rib. By week 12, she reached her final status. At the same time as this migration, the morphology of the scapula changes: from wider than high at the start, its dimensions are gradually reversed to reach definitive dimensions, higher than wide, due to the adaptation of this bone to bipedalism and the gripping function of the upperlimb.
The congenital elevation of the scapula would therefore result from an arrest of the caudal migration of this structure between the 9th and 12th weeks. This stopping of the migration of the scapula is also associated with a stopping of development of the neighboring soft parts, in particular of the muscles which insert themselves on the scapula (rhomboid, angular and trapezius), often hypoplastic or even fibrous and infiltrated with fatty tissue [2]. In 20 to 30% of patients, an omovertebral bone is found, either made up of bone, cartilage or fibrous tissue, between the upper angle of the scapula and the spinous process of the cervical vertebrae [3]. A few familial forms have been described and suggest the possibility of genetic transmission [4].
Sprengel’s deformity is generally unilateral (90% of cases), more common in girls than in boys (sex ratio of 1:3) with or without left or right predominance. It is often diagnosed early in childhood. Parents consult for unsightly disfigurement (scapular asymmetry, posterior thoracic swelling corresponding to the projection of the point of the scapula) and / or limited active lifting of the shoulder [5]. The Cavendish classification differentiates between four clinical grades of increasing severity, depending on the size of the swelling and the elevation of the scapula, from a very slight malformation (grade 1) to a severe malformation (grade 4).
Grade I (very light): Level shoulders and strainal most invisible when the patient is dressed.
Grade II (mild): Shoulders practically level, but the deformity is visible when the patient is dressed.
Grade III (moderate): Shoulder 2 to 5 cm raised and the deformity is easily visible.
Grade IV (severe): Shoulder significantly elevated, with the superior angle of the scapula close to the occipital [6].
Antenatal ultrasound was able to detect omovertebral bone in a fetus with asymmetric thickening of soft nuchal tissue [1]. Postnatal radiography is essential for diagnosis despite the technical difficulties in visualizing the bone. In addition to the degree of elevation on an X-ray standing with arms hanging down to the side of the body, it can show the presence of omovertebral bone and indicate the extent of bone hypoplasia [2]. The CT scan and its 2D and especially 3D reconstructions are very useful for finding the omovertebral bone and specifying the location and size, evaluating the position of the scapula in space and the extent of scapular dysmorphia, looking for associated bone abnormalities, especially vertebral. However, in the preoperative assessment, it does not make it possible to satisfactorily assess a possible non-ossified component or the presence of a fibrous or cartilaginous structure, hence the interest of MRI to analyze this fibrous component and / or cartilage and on the other hand to look for associated bone marrow abnormalities such as diastematomyelia [4].
Conclusion
Sectional imaging is essential for the diagnosis of Sprengel’s deformity; computed tomography with multiplanar reconstructions studies the anatomical features of bone structures while MRI analyses the spinal cord and its environment.
Declarations
Competing interests: The authors declare no conflict of interest.
Contributions from authors: All the authors contributed to the conduct of this work. They also state that they have read and approved the final version of the manuscript.
References
- Chinn DH. Prenatal ultrasonographic diagnosis of Sprengel’s deformity. Journal of Ultrasound in Medicine. 2001; 20: 693–697. https://doi.org/10.7863/jum.2001.20.6.693.
- Mallet JF, Bronfen C. Malformations de la ceinture scapulaire chez l’enfant et l’adolescent. EMC - Appareil locomoteur. 2006; 1: 1–7. https://doi.org/10.1016/S0246-0521(02)00126-2.
- Walstra FE, Alta TD, van der Eijken JW, Willems WJ, Ham SJ, et al. Long-term follow-up of Sprengel’s deformity treated with the Woodward procedure. Journal of Shoulder and Elbow Surgery. 2013; 22: 752–759. https://doi.org/10.1016/j.jse.2012.08.014.
- Guillaume R, Nectoux É, Bigot J, Vandenbussche L, Fron D, et al. Surélévation congénitale de la scapula (déformation de Sprengel): A propos de quatre cas. Journal de Radiologie Diagnostique et Interventionnelle. 2012; 93: 928–933. https://doi. org/10.1016/j.jradio.2012.07.007.
- Rasul M, Reddy A. The sprengel deformity. Int J Res Med Sci. 2015; 38: 69–71. https://doi.org/10.18203/2320-6012. ijrms20151457.
- Elzohairy MM, Salama AM. Sprengel’s deformity of the shoulder joint treated by Woodward operation. Eur J Orthop Surg Traumatol. 2019; 29: 37–45. https://doi.org/10.1007/s00590-018- 2291-y.