
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
SARS CoV2 double mutant variant causing CT changes in chest with rapid fall in oxygen saturation: Rationale for havoc in second wave in India
Pooja Das1; Ayush Pandey2; Poonam Kumar Saidha3*; Sahil Kapoor4; Mithun Abraham5; Vikas Kakkar6
1 Department of ENT, Post graduate Resident, SGT University, Gurugram, India.
2 Department of Pulmonary Medicine, Post graduate Resident, SGT University, Gurugram, India.
3 M.S ENT, Department of ENT, Associate Professor, SGT University, Gurugram, India.
4 M.S ENT, Department of ENT, Assistant Professor, SGT University, Gurugram, India.
5 M.S ENT, Department of ENT, Senior Resident, SGT University, Gurugram, India.
6 M.S ENT, Department of ENT, Professor & HOD, SGT University, Gurugram, India.
*Corresponding Author: Poonam Kumar Saidha
M.S ENT, Department of ENT, Associate Professor,
SGT University, Gurugram, India.
Email: poonamsaidha@gmail.com
Received : Dec 23, 2021
Accepted : Feb 16, 2022
Published : Feb 23, 2022
Archived : www.jcimcr.org
Copyright : © Saidha PK (2022).
Abstract
Background: Explore the cause of rapid advancing nature of double mutant strain in Indian Population especially in Northern Province and to access the deterioration of the patient’s condition from day 1 of admission to rapid decline in oxygen saturation with gross lung involvement noticed in CT Chest reports.
Methods: The study was conducted in COVID 19 Ward and ICU at a tertiary care hospital in Gurgaon. A total of 60 patients were selected who were RT-PCR positive, all the patients were evaluated with continuous vitals monitoring and treatment.
Results: From 60 patients, 35 patients showed rapid deterioration with fluctuating SpO2 and significant lung changes in CT chest whereas rest of 25 patients were maintaining SpO2 at 96% in room air. These sick patients were found to be falling in the young and middle age population who were non vaccinated and some had comorbidities as well on irregular medication.
Conclusion: Our study aims to focus on the symptomatology and progress of the virus causing significant lung parenchymal involvement encountered specifically in the younger populations, most likely due to the undergoing genetic mutation of the virus thereby increasing transmissibility and virulence responsible for rise in number of mortality rates.
Keywords: B.1.617 lineage; CORADS; mutant strain; SARS- CoV-2; virulence.
Citation: Das P, Pandey A, Saidha PK, Kapoor S, Abraham M, et al. SARS CoV2 double mutant variant causing CT changes in chest with rapid fall in oxygen saturation: Rationale for havoc in second wave in India. J Clin Images Med Case Rep. 2022; 3(2): 1689.
Introduction
COVID-19 is an infection that has spread worldwide becoming a pandemic with enormous ramifications for the sociopolitical environment and healthcare delivery system [1]. The clinical presentations ranged from asymptomatic carriers to patients requiring mechanical ventilation, and ICU hospitalizations with higher mortality making it a rare and unanticipated concern [2,3].
In October 2020, a new variant was discovered in India which was named B.1.617. There were very few detections until January 2021 but by April it had spread to at least 20 countries [4-6]; Among some 15 defining mutations, it has spike mutations D111D (synonymous), G142D [7], P681R, E484Q [8] and L452R [9], the latter two of which may cause it to easily avoid antibodies [10]. In an announcement on 15 April 2021, Public Health England (PHE) designated B.1.617 as a ‘Variant under investigation’, VUI-21APR-01 [11]. On 29 April 2021, PHE added two further variants, VUI-21APR-02 and VUI-21APR-03, effectively B.1.617.2 and B.1.617.3. [12] British scientists declared B.1.617.2 (which notably lacks mutation at Spike E484) as a “variant of concern”, after they flagged evidence in early May 2021 that it spreads more quickly than the original version of the virus [13,14].
A non-contrast high-resolution CT chest imaging serves a critical role in early illness diagnosis, particularly in patients with false-negative RT-PCR findings, as well as in disease management and monitoring [15]. Furthermore, the imaging data may be used to determine the severity of the condition, which greatly aids doctors in their clinical judgement and ensures appropriate and prompt care [16]. An increasing rate of infection of the mutant strain have come forward where majority of the population falls in the range of early 30s to late 40s, with an expeditious respiratory failure where patients become dependent on oxygen supplementation. Our study highlights the virulence and transmissibility of the double mutant strain particularly in the younger and middle aged populations and its progress from upper respiratory tract to lower respiratory tract specifically the lungs resulting in rapid deterioration with fall in SpO2 levels and the role of vaccination on this strain
Materials and methods
Aim and objectives
1) To explore the cause of rapid advancing nature of double mutant strain in Indian Population specially in Northern province.
2) To access the deterioration of patients from day 1 of admission to rapid decline in oxygen saturation with HRCT Chest findings.
3) Role of Vaccination on the mutant strain of SARSCOV-2.
Study design
Clinical research study (Observational study in epidemiology) of 60 patients who were laboratory tested RT-PCR positive for SARS CoV- 2 Virus.
Study setting
The study was conducted in the month of April-May 2021in COVID 19 Ward and COVID designated ICU at a tertiary care hospital in Gurgaon, India.
Institutional ethical committee: Clearance Approved. Inclusion criteria 1) Patient age above 18 years 2) Symptomatic cases who were RT- PCR laboratory confirmed positive for SARS-CoV-2 3) Patient presenting with all the prodromal symptoms entitled for COVID -19 with sore throat, anosmia, shortness of breath, low oxygen saturation and/or chest pain.
Exclusion criteria 1) Patient age below 18 years 2) Asymptomatic cases 3) Patient who were diagnosed with any respiratory or cardiac co-morbidities like COPD, ILD, CAD, RHD prior to COVID 19 infection 4) Any history of cardiac surgery
CO-RADS based on the CT findings
The level of suspicion of COVID-19 infection is graded as CORADS score [17]: CO-RADS 1: COVID-19 is extremely improbable, CT is normal, or results suggest a non-infectious condition; CO-RADS 2: There is little reason to suspect COVID-19 infection, and CT results are compatible with other infections. CO-RADS 3: COVID-19 infection is unclear or ambiguous, and CT abnormalities suggest infection but do not rule out COVID-19 involvement; CORADS 4: the level of suspicion is strong, and the majority of CT results are suspicious but not particularly typical, such as unilateral ground glass, confluent, or multifocal consolidations without a typical position or any other characteristic findings; and CO-RADS 5: with usual CT results, the threshold of suspicion is hig CO-RADS 6: RT-PCR positive.
Results
Demographic, severity, and clinical characteristics
In this clinical research study total of 60 patients were enrolled who were laboratory confirmed RT-PCR positive for SARSCOV-2. Selected patients comprised of 35 male and 25 female patients from which 46 patients were below 50 years and 14 patients were above 50 years of age. Co-morbidities like hypertension, and diabetes mellitus were observed in total 31 patients. All the 60 patients presented with mild fever, sore throat and anosmia, few had wheezy breathing. These patients were admitted to COVID wards and all of them were subjected to full clinical data collection including age, gender, exposure history, clinical complaint, and laboratory parameters along with regular vital monitoring. These patients underwent complete ENT examination including Diagnostic nasal endoscopy carrying all precautionary measures of wearing PPE kits. On admission all the patients showed baseline SpO2 of 91-95%. Sudden decline of SpO2 to 65-70% was observed in 35 patients on third to fourth day of admission with progressive difficulty in breathing and tachycardia (Figure 1). These sick patients were segregated and shifted to COVID ICU where prompt oxygen inhalation with other I.V medication were started at once and there maining 25 patients who showed no fluctuation in SpO2 were labelled as mild group and consecutively shifted to COVID ward. The sick patients maintained SpO2 to 85-90% at 5 liters of oxygen belonged to the moderate-severe group. Majority of these patients were falling in the young & middle aged populations who were non-vaccinated and showed a rapid deterioration of symptoms with fall in SpO2 in a span of 3-5 days (As illustrated in Table 1).
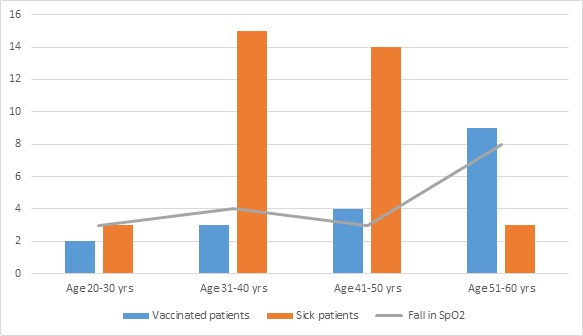
Table 1:Showing duration of fall in spo2 in sick patients correlating with the vaccination status.
Age in years |
No of Patients |
Co-morbidities |
Vaccination |
Sick patients |
Average Duration of fall in SpO2 from day 1 of admission |
||||
|
|
|
Hypertension |
Diabetes mellitus |
|
YES |
NO |
|
|
20-30 |
14 |
00 00 |
02 12 |
03 |
3 days |
||||
31-40 |
18 |
06 04 |
03 15 |
15 |
4 days |
||||
41-50 |
14 |
06 03 |
04 10 |
14 |
3 days |
||||
51-60 |
14 |
08 04 |
09 05 |
03 |
8 days |
||||
Total |
60 |
20 11 |
18 42 |
35 |
|
||||
CT imaging findings
Chest CT findings were assessed and analysed for all patients falling in moderate to severe group. Majority of the cases presented with bilateral involvement with peripheral and lower lobe predominance (Figure 2.1). According to the CT findings, the most prominent features are ground glass opacities with vascular pleural thickening and interlobularseptations were the most constant imaging features (Figure 2 and 2.2). According to the CO-RADS classification, 3 patients was classified as CO-RADS 3, 7 patients showed CO-RADS 4 findings, and 25 patients were classified as CO-RADS 5. The CT-Severity score were from 1 to 25, with a mean value of 7 and a median value of 7. Among all 35 sick patients, 3 had CT-SS of 1-5, 7 had CT-SS of 6-10, 12 had CT-SS of 11–15, 10 had CT-SS of 16-20 and 3 had CT-SS of 21-25 (Table 2). Patients falling in moderate and severe category were given treatment as per the COVID 19 management protocol.



Table 2:Number of cases in each severity score group (n=35).
CT severity score |
CO-RADS |
Number of cases |
Percentage |
1-5 |
3 |
3 |
8.57 |
6-10 |
4 |
7 |
20 |
11-15 |
5 |
12 |
34.28 |
16-20 |
5 |
10 |
28.57 |
21-25 |
5 |
3 |
8.57 |
Discussion
COVID-19 is a highly infectious disease that has been spreading widely worldwide. Early diagnosis is an essential disease management strategy [18]. The most common clinical symptoms of patients with COVID-19 are fever, cough, dyspnoea, and fatigue [19]. Lineage B.1.617 is one of the known variants of SARS-CoV-2 was first identified in Maharashtra, India on 5 October 2020 [20,21]. It has been referred to as a double mutation variant [22,5,23]. “Double mutation” refers to B.1.617’s mutations in the gene encoding the SARS-CoV-2 spike protein [24] causing the substitutions E484Q and L452R [25]. Emerging research suggests the variant may be more transmissible than previously evolved ones [26].
Characteristics
Surveillance data from the Indian government’s Integrated Disease Surveillance Programme (IDSP) shows that around 32% of patients, both hospitalised and outside hospitals, were aged below 30 in the second wave compared to 31% during the first wave. The data also showed a higher proportion of asymptomatic patients were admitted during the second wave, with more complaints of breathlessness [27]. On 7 May 2021, British scientists at Public Health England (PHE) re-designated one of the three sub-lineages, B.1.617.2, as “variant of concern” (VOC21APR-02) [28], after they flagged evidence in May 2021 that it spreads more quickly than the original version of the virus. Another reason was that they identified 48 clusters of B.1.617.2, some of which revealed a degree of community transmission [13,29]. Despite its designation, B.1.617.3 was the first sub-lineage of this variation to be discovered in India in October 2020. This sub-lineage has remained uncommon in comparison to the two other sub-lineages, B.1.617.1 and B.1.617.2, both of which were discovered in December 2020, both of which were first detected in December 2020 [30]. There were few known cases of B.1.617 (of all sub-lineages) until early February 2021 when there was a significant increase [22]. The PHE considers the sub-lineages B.1.617.1 and B.1.617.3 as “variants under investigation” under the names VUI-21APR-01 and VUI-21APR-03, while B.1.617.2 was upgraded to a “variant of concern” under the name VOC-21APR-02 (previously VUI-21APR-02) on 7 May 2021[31].
Vaccine efficacy
ICMR found that convalescent sera of the COVID-19 cases and recipients of Bharat Biotech’s BBV152 (Covaxin) were able to neutralise VUI B.1.617 although with a lower efficacy [32]. The most current study looked at convalescent Sera of COVID-19 patients and persons who had the Covaxin vaccination, which is utilised in India. It was discovered to be capable of neutralising the 617 versions [33]. Viruses, in general, accumulate mutations throughout time, giving rise to new types. An “emerging variation” is a novel variety that appears to be increasing in a population.
The following are some of the probable repercussions of developing variations [34,35]: • Increased transmissibility • Increased morbidity • Increased mortality • Ability to evade detection by diagnostic tests • Decreased susceptibility to neutralizing antibodies, either therapeutic (e.g., convalescent plasma or monoclonal antibodies) or in laboratory experiments • Ability to evade natural immunity (e.g, causing reinfections) • Ability to infect vaccinated individuals • Increased risk of particular conditions such as multisystem inflammatory syndrome or long-haul COVID • Increased affinity for particular demographic or clinical groups, such as children or immunocompromised individuals
Variants that appear to match one or more of these criteria may be labelled “variants under study” or “variants of interest” until their attributes are verified and validated [36]. More research is being performed to learn more about the B.1.617 (double mutant) strain. For diagnosing COVID-19 pneumonia, laboratory studies were the gold standard. However, they are occasionally inaccessible in an emergency, and the findings are not instantly available [37]. After a mean delay of 5 days, a chest CT showed a 97 percent sensitivity for the diagnosis of COVID-19 pneumonia [37]. Because it measures the depth and severity of the disease, which might indicate the disease burden, chest CT could be a useful supplement for disease diagnosis [19].
The CT-SS of COVID-19 pneumonia is extremely useful in determining the extent of pneumonia involvement, distinguishing moderate, severe, and critical kinds, and predicting the dynamic changes of chest CT follow-up exams in different severities of COVID-19 pneumonia. Furthermore, determining the severity of COVID-19 at an early stage allows doctors to treat the condition more effectively and efficiently [38]. Tachypnoea, hypoxemia, and infiltration of more than 50% of the lung fields are signs of severe illness [39]. The best CT-SS threshold for detecting severe COVID-19, according to Yang et al. [19] was 19.5/40, with 83.3 percent sensitivity and 94 percent specificity. Furthermore, Francone et al. [40] found that a CT-SS of 18 is highly predictive of patient death in a short-term follow-up.
In our study, fever and lower respiratory symptoms are the most common presenting complaints. It has been observed that in January early 2021 the infection rate of COVID 19 have showed to an insidious rise affecting the younger generations more commonly. The symptoms presentation although remains the same as fever, cough, sore throat and dyspnoea but the patients experience mild symptoms of fever and cough which subsides with medication and in a span of 4-5 days then they start experiencing shortness of breath with fluctuating SpO2 ranging from 84-91%. This have caused a havoc among general populations as they have to rely on oxygen inhalation for their optimum respiration. Many studies have been conducted and are still on the process to explore the reason behind this extensive virulence and transmissibility of the mutant virus strain and the role of vaccination on this mutant strain.
Conclusion
An unexpected speedy rise of COVID 19 is causing an alarming state globally but affecting India at a wider range. As per the studies conducted so far it has been observed that the virulence and contagiosity of the virus is because of the emergence of the double mutant strain of the virus due to its continuous genetic mutation. Our study exhibits, the virulent nature of this mutant strain and its rapid advancement from the nasal cavity/ nasopharynx (portal of viral entry) causing milder symptoms at an initial stage which in a few days results in rapid deterioration with fluctuating SpO2 level and gross lung parenchymal involvement. Such scenario compels the patient to be reliant on oxygen for survival. The incidence of such cases in our study has been encountered in young and middle aged populations with a poor vaccination rate.
Declarations
Acknowledgement: I wish to express my sincere gratitude to my HOD and my senior faculties for their guidance and encouragement in carrying out this research work during such a stressful situation amid Pandemic. This research article is a multi-disciplinary team work supported and executed by coordination of ENT & Respiratory Medicine Department. I would like to thank the paramedical and nursing staffs for their cooperation.
Declaration of conflicting interests by authors: None
References
- http://www.who.int.https://www.who.int/emergencies/diseases/novel-coronavirus-2019?gclid=EAIaIQobChMImt2m3afS 6wIVvSB7Ch3xdQDoEAAYASAAEgLb-_D_BwE Coronavirus Disease (COVID-19)—World Health Organization.
- Emedicine.medscape.com, Coronavirus Disease 2019 (COVID-19) Clinical Presentation: History, Physical Examination, Complications, https://emedicine.medscape.com/ article/2500114- clinical.
- Thomas Ruddel D, Winning J, Dickmann P, et al. Coronavirus disease 2019 (COVID-19): Update fur an asthesisten und intensivmedizinermarz 2020. Der Anaesthesist. 2020; 69: 225.
- PANGO lineages. cov-lineages.org. Retrieved 18 April 2021.
- Koshy J (8 April 2021). Coronavirus | Indian ‘double mutant’ strain named B.1.617. The Hindu.
- India’s variant-fuelled second wave coincided with spike in infected flights landing in Canada. Toronto Sun. 2021; Retrieved 10 April 2021.
- Cherian Sarah, Potdar Varsha, Jadhav Santosh, Yadav Pragya, Gupta Nivedita, et al. (24 April 2021). Convergent evolution of SARS-CoV-2 spike mutations, L452R, E484Q and P681R, in the second wave of COVID-19 in Maharashtra, India. S2CID 233415787. Retrieved 25 April 2021.
- Shrutirupa (17 April 2021). Is This COVID–20? | Double Mutant Strain Explained. Self Immune. Retrieved 18 April 2021.
- Double mutant: What are the risks of India’s new Covid-19 variant. www.bbc.co.uk/news. 25 March 2021. Retrieved 11 April 2021.
- Haseltine WA. An Indian SARS-CoV-2 Variant Lands In California. More Danger Ahead? Forbes.com, Apr 12, 2021, accessed 14 April 2021
- Confirmed cases of COVID-19 variants identified in UK (see: Thursday 15 April/New Variant Under Investigation (VUI) designated). www.gov.uk. 15 April 2021. Retrieved 16 April 2021.
- Confirmed cases of COVID-19 variants identified in UK (see: Two VUIs added to B.1.617 group). www.gov.uk. 29 April 2021. Retrieved 1 May 2021.
- British scientists warn over Indian coronavirus variant. Reuters. 7 May 2021. Retrieved 7 May 2021.
- SARS-CoV-2 variants of concern as of 6 May 2021. European Centre for Disease Prevention and Control. Retrieved 12 May 2021.
- J Liu, H Yu, S Zhang. The indispensable role of chest CT in the detection of coronavirus disease 2019 (COVID-19). European Journal of Nuclear Medicine and Molecular Imaging. 2020; https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC71187 04/#CR2, In press.
- Bernheim A, Mei X, Huang M, et al. Chest CT findings in coronavirus disease-19 (COVID-19): Relationship to duration of infection. Radiology. 2020; 295: 200463.
- COVID working group of the Dutch Radiological Society. 25-3- 2020.
- Chung M, Bernheim A, Mei X, et al. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiol. 2020; 295: 202 –207.
- Yang R, Li X, Liu H, et al. Chest CT severity score: an imaging tool for assessing severe COVID-19. Radiol Cardiothorac Imaging 2:2.
- Tracking of Variants. gisaid.org. GISAID. 26 April 2021. Retrieved 13 May2021.
- Expert reaction to cases of variant B.1.617 (the ‘Indian variant’) being investigated in the UK. Science Media Centre. Science Media Centre. Retrieved 20 April 2021.
- PANGO lineages Lineage B.1.617. cov-lineages.org. Retrieved 11 May2021.
- Cuff, Madeleine (19 April 2021). Indian variant: Cases of new ‘double mutation’ Covid strain thought to be spreading in UK. i. London. Retrieved 20 April 2021.
- Shang Jian, Yushun Wan, Lou Chuming, Ye Gang, Geng Qibin, et al. Cell entry mechanisms of SARS-CoV-2. Proceedings of the National Academy of Sciences. 2020; 117: 11727–11734.
- Starr Tyler N, Greaney Allison J, Dingens Adam S, Bloom Jesse D. (April 2021). Complete map of SARS-CoV-2 RBD mutations that escape the monoclonal antibody LY-CoV555 and its cocktail with LY-CoV016. Cell Reports Medicine: 100255.
- Deng Xianding, Garcia-Knight Miguel A, Khalid Mir M, Servellita Venice, Wang Candace, et al. Transmission, infectivity, and neutralization of a spike L452R SARS-CoV-2 variant. Cell. 2021; 0. ISSN 0092-8674. Retrieved 26 April 2021.
- Dey Sushmi. Covid second wave in India: Percentage of young infected in second wave same, but more serious. The Times of India. Retrieved 27 April 2021.
- SARS-CoV-2 variants of concern and variants under investigation in England - Technical briefing 10 (PDF) (Report). London. Public Health England. 7 May 2021. Retrieved 7 May 2021.
- Davis, Nicola (7 May 2021). Indian Covid variant is ‘of concern’, says Public Health England. The Guardian. London. Retrieved 7 May 2021.
- Weekly epidemiological update on COVID-19 - 27 April 2021. World Health Organization. 27 April 2021. Retrieved 28 April 2021.
- Confirmed cases of COVID-19 variants identified in UK. www. gov.uk. 7 May 2021. Retrieved 8 May 2021.
- Yadav, Pragya D, Sapkal, Gajanan N. Neutralization of variant under investigation B.1.617 with sera of BBV152 vaccinees (PDF). Retrieved 24 April 2021.
- Covaxin found to neutralise 617 variant of COVID-19, says Dr.Fauci. The Hindu. 2021.
- Emerging SARS-CoV-2 Variants. cdc.org (Science brief). Centers for Disease Control and Prevention. 2021. Retrieved 4 January 2021. This article incorporates text from this source, which is in the public domain.
- IDSA Contributor (2 February 2021). COVID Mega-variant and eight criteria for a template to assess all variants. Science Speaks: Global ID News. Retrieved 20 February 2021.
- Variants: distribution of cases data. gov.uk. Government Digital Service.
- Hani C, Trieua NH, Saaba I, Dangearda S, Bennani S, et al. 2020; COVID-19 pneumonia: A review of typical CT findings and differential diagnosis. Diagn Inter Imaging. 101: 263-268.
- Liu N, He G, Yang X, et al. Dynamic changes of chest CT follow-up in coronavirus disease-19 (COVID-19) pneumonia: relationship to clinical typing. BMC Med Imaging. 2020; 20: 92.
- Gandhi RT, Lynch JB Carlos del Rio. Mild or moderate Covid-19. N Engl J Med. 2020; 1-9.
- Francone M, Iafrate F, Masci GM, et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur Radiol. 2020; 4: 1-10.