
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Acute sacroiliitis in acne fulminans
Fadi Kharouf1*; Yusef Azraq2; Yuval Ishay3; Issam Hindi1
1 Department of Medicine, Rheumatology Unit, Hadassah Medical Organization, Faculty of Medicine, Hebrew University of Jerusalem, Israel.
2 Department of Diagnostic Radiology, Hadassah Medical Organization, Faculty of Medicine, Hebrew University of Jerusalem, Israel.
3 Department of Medicine, the Institute of Gastroenterology and Liver Diseases, Hadassah Medical Organization, Faculty of Medicine, Hebrew University of Jerusalem, Israel.
*Corresponding Author: Fadi Kharouf
Department of Medicine, Rheumatology Unit,
Hadassah Medical Organization, Faculty of Medicine, Hebrew University of Jerusalem, Israel, Kiryat
Hadassah, POB 12000, Jerusalem 91120, Israel.
Email: fadikharouf@hotmail.com
Received : Jan 21, 2022
Accepted : Feb 17, 2022
Published : Feb 24, 2022
Archived : www.jcimcr.org
Copyright : © Kharouf F (2022).
Abstract
A 19-year-old male patient presented with a 2-week history of right hip and buttock aches. His past medical record was unremarkable, except for severe diffuse acne, for which he was recently started on isotretinoin. Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) scans displayed changes consistent with active sacroiliitis. While therapy with non-steroidal anti-inflammatory drugs achieved no benefit, prednisone led to remarkable recovery. The acute presentation, the severe acne, the temporal association with the use of isotretinoin, and the response to corticosteroids are compatible with the diagnosis of acne fulminans.
Abbreviations: CT: Computed Tomography; MRI: Magnetic Resonance Imaging.
Citation: Kharouf F, Azraq Y, Ishay Y, Hindi I. Acute sacroiliitis in acne fulminans. J Clin Images Med Case Rep. 2022; 3(2): 1693.
Description
A 19-year-old male patient presented with a 2-week history of right hip and buttock aches. His past medical record was unremarkable, except for severe diffuse acne (Figure 1), for which he was recently started on isotretinoin.

Physical examination was notable for lumbosacral tenderness, along with a positive FABER test, and pain upon right hip internal rotation. Inflammatory markers were high, and serology for brucella subtypes was negative.
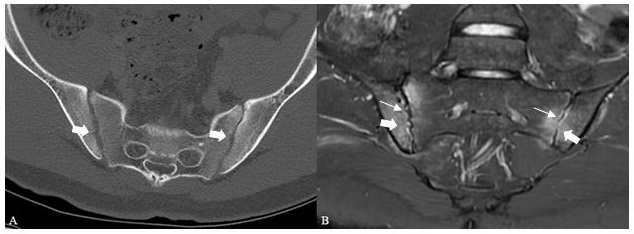
Pelvic Computed Tomography (CT) scan showed sacroiliac joint erosions, more prominent on the right side, with joint space pseudo-widening (Figure 2A). The patient was treated with painkillers and non-steroidal anti-inflammatory drugs. In light of his lack of response to therapy, pelvic Magnetic Resonance Imaging (MRI) scan was performed, revealing bilateral sacroiliac bone marrow edema and erosions (Figure 2B), compatible with osteitis. To further explore the extent of the disease, bone scan was done, displaying increased radiotracer uptake in the sacroiliac joints and trochanteric bursae.
The combination of severe acne, recent isotretinoin therapy, and osteitis on imaging, raised suspicion for acne fulminans, probably isotretinoin-induced. Prednisone, 30 mg, led to prompt recovery.
Acne fulminans is an uncommon variant of inflammatory acne. It is characterized by the rapid development of painful erosions and hemorrhagic crusts, resulting in severe scars. In extreme cases, the disorder can manifest as systemic inflammation, with fever, arthralgia, and osteolytic bone lesions. Isotretinoin therapy is a potential trigger of the disease, especially when started at high doses [1].
Recognition of such entity is essential for avoiding misdiagnoses, such as ankylosing spondylitis and septic arthritis.
Disclosure: The authors have no conflict of interests to declare.
References
- Greywal T, Zaenglein AL, Baldwin HE, Bhatia N, Chernoff KA, et al. Evidence-based recommendations for the management of acne fulminans and its variants. J Am Acad Dermatol. 2017; 77: 109.