
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Endovascular treatment for postoperative cerebral embolism after video-assisted thoracic surgery: Report of 3 cases and literature review
Jiangshan Deng1; Yueqi Zhu2; Yuwu Zhao1*
1 Department of Neurology, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai 200233, China.
2 Department of Radiology, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai 200233, China.
*Corresponding Author: Yuwu Zhao
Department of Neurology, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai
200233, China.
Email: zhaoyuwu2005@126.com
Received : Jan 27, 2022
Accepted : Feb 21, 2022
Published : Feb 28, 2022
Archived : www.jcimcr.org
Copyright : © Zhao Y (2022).
Abstract
Postoperative cerebral embolism after video-assisted thoracic surgery is a severe complication. However, it is still unclear how the cerebral embolism developed after operation, and how can we treat the stroke and prevent further embolism. We present three cases suffering cerebral embolism after lung surgery transferred from another chest hospital. All of them underwent endovascular thrombectomy and discharged with proper recovery. Endovascular thrombectomy is effective for cerebral embolism after video-assisted thoracic surgery.
Keywords: cerebral embolism; perioperative stroke; endovascular thrombectomy; pulmonary lobectomy; video-assisted thoracic surgery
Citation: Deng J, Zhu Y, Zhao Y. Endovascular treatment for postoperative cerebral embolism after video-assisted thoracic surgery: Report of 3 cases and literature review. J Clin Images Med Case Rep. 2022; 3(2): 1697.
Introduction
The rate of death and disability from perioperative stroke is high. Patients with postoperative stroke have a great risk of death or severe disability upon discharge from the hospital [7,12]. Most perioperative strokes are ischemic. Although the role of endovascular therapy in patients with acute large vascular occlusion has been demonstrated, the data on perioperative stroke in hospitalized patients is limited. At present, thoracic interventional diagnosis and treatment technology is widely used in clinical practice. We reported three cases of cerebral infarction after video-assisted thoracic surgery on the lungs, obtained good functional outcomes after mechanical thrombectomy in the emergency, aiming to emphasize on the perioperative stroke associated with thoracic interventional treatment, and to confirm the effectiveness of emergent endovascular treatment for the disease. The review of previous reported and our patients’ characteristics are listed in the table 1 [6,9,14,16].
Table 1: Patients’ characteristics.
|
Our case 1 |
Our case2 |
Our case3 |
Daisuke Kimura |
Daisuke Kimura |
Yusuke Morinaga |
Yusuke Morinaga |
Eri Shiozaki |
Genki Usui |
Sex |
F |
F |
M |
M |
F |
M |
M |
M |
M |
Age |
23 |
54 |
67 |
76 |
67 |
71 |
76 |
73 |
68 |
Hypertension (Y/N) |
N |
N |
Y |
NA |
NA |
Y |
Y |
Y |
Y |
Diabetes (Y/N) |
N |
N |
N |
NA |
NA |
N |
N |
N |
Y |
Atrial Fibrillation (Y/N) |
N |
N |
Y |
Y |
N |
N |
N |
Y |
N |
Surgery type |
PNR |
PNR |
LUL |
LUL |
LLL |
LUL |
LUL |
LUL |
LLL |
Time after surgery |
12h |
3d |
10h |
2d |
4d |
0d |
6d |
19d |
27h |
Location of cerebral artery |
LMCA-M1 |
LICA-T |
RICA-T |
RMCA |
LMCA |
LMCA-M3 |
LMCA-M1 |
RMCA-M1 |
LMCA-M1 |
Baseline NIHSS |
22 |
23 |
10 |
NA |
NA |
22 |
20 |
17 |
24 |
TICI(Post recanalization) |
3 |
2b |
2b |
3 |
3 |
2b |
3 |
2b |
2b |
mRS(3M) |
0 |
3 |
2 |
0 |
1 |
2 |
2 |
3 |
0 |
PNR: Pulmonary nodule resection. LUL: Left upper lobectomy. LLL: Left lower lobectomy. MT: Mechanical thrombectomy.
Case 1
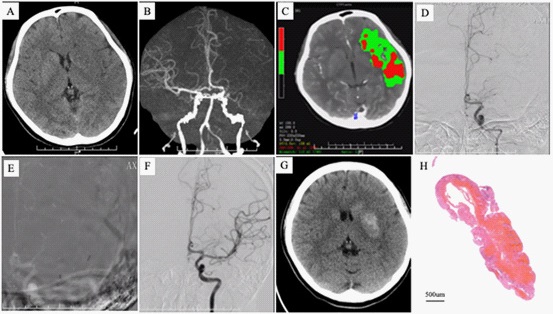
A 23-year-old girl underwent video-assisted pulmonary nodule resection (PNR) in the morning in another chest hospital. She fell asleep at 21:20 PM and was found restless, unable to communicate, right limbs and legs weakness half an hour later. She was transferred to our stroke center by the ambulance at 3:08 AM the next morning. A quick neuro examination found she was stupor and dysphoria, right complete hemiplegia, mixed aphasia, conjugate deviation of the eyes to the left, (Glasgow Coma Scale, 8 points [E2V2M4]). The National Institutes of Health Stroke Scale (NIHSS) was 22 points. Multi model computer scan showed no cerebral hemorrhage and occlusion at proximal M1 segment of left middle cerebral artery. CT perfusion showed extensive low perfusion of the area supplied by left middle cerebral arterial (Figure 1). Metrics calculated by MIStar software were rCBF volume <30%: 41 ml, Mismatch volume: 115 ml, DT>3s: 156 ml, Mismatch ratio: 3.8. Electrocardiogram examination showed normal sinus rhythm. D dimer: 3.18 mg/L. The patient was diagnosed with acute cerebral infarction and underwent emergent endovascular treatment. Briefly, the patient was placed a long artery sheath (6F, 90 cm) on the right femoral artery under local anesthetic. Then a reperfusion catheter (ACE 60, Alameda, California) was brought into the left internal carotid artery and closure of the left proximal M1was verified by angiography. Subsequently, through the intermediate catheter, the microcatheter (Rebar 27, ev3) was navigated to the distal left MCA artery guided by the micro guiding wire (Synchro2, Stryker). EmboTrap II retriever (5 X 33 mm, Cerenovus) was used to remove the thrombus with Solumbra technique. Complete recanalization was achieved after the first pass of thrombectomy. The blood flow was graded TICI 3 (Figure 1). The symptom of the patient alleviated quickly. The NIHSS was 4 points 9 h after the operation. A series of computer scan conducted to follow up in the next few days (Figure 1). Histology examination showed mixed fibrinogen with red cells and granulocytes in the thrombus (Figure 1). During the hospitalization, laboratory test showed a sinus rhythm, normal heart valve structure. Contrast echocardiography of right heart didn’t find right-to-left shunt and patent foramen ovale. Anti-O, serum rheumatic factors, anticyclic peptide antibodies, anti-nuclear antibodies, anti-dsDNA antibodies, perinuclear antineutrophil cytoplasmic antibody (pANCA), cytoplasmic antinuclear cytoplasmic antibody (cANCA) were all negative in the plasma. The patient received glycerin fructose dehydration from the next day and initiation of anticoagulant with low-molecular heparin on the fourth day after operation. She was charged on the tenth day after operation with minor facial paralysis. Follow up in 3 months showed none symptom, NIHSS: 0 points and mRS: 0 points.
Case 2
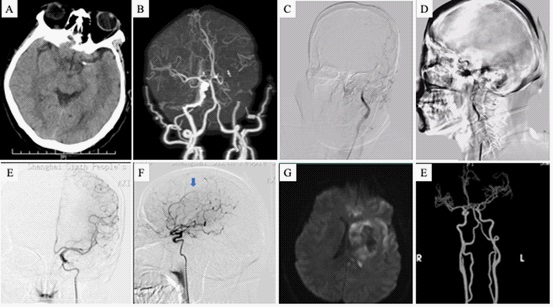
A 54-year old female was treated with video-assisted pulmonary nodule excision. Three days later, there was a sudden onset of weakness in her right limbs and slurred speech. She was transferred to our stroke center by ambulance 115 minutes later. Nervous system physical examination showed she was in drowsiness, conjugate deviation of the eyes to the left, mixed aphasia, shallow nasolabial groove on the right, muscle strength of the left limb grade V and the right limb grade 0, NIHSS: 23 points. This patient has no history of hypertension, diabetes and heart disease. Computer scan showed no cerebral hemorrhage and occlusion of left internal carotid artery. DSA showed the occlusion located at distal T terminal. The Solumbra technique used same as in the procedure of the first patient. Intermediate catheter (6 F, 105 cm, Navein) and Solitaire stent AB (4 X 20 mm) were used in the procedure. Recanalization of the artery was achieved after four times of manipulation. A fraction of thrombus escaped and run to the pericallosal artery. The reperfusion status was graded TICI 2b (Figure 2). There was infraction with some hemorrhage classified to HI2 according to ECASS II criteria (Figure 2). This patient was treated with atorvastatin and delayed antiplatelet drug. She was charged 14 days after operation and transferred to a rehabilitation hospital. Follow-up showed she got a recovery with a mRS 3 in 3 months, and mRS 2 in 6 months.
Case 3
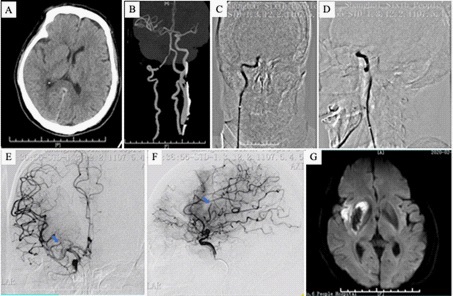
A 67-year old smoking male underwent video-assisted left upper lobectomy for lung cancer in the morning. He has a history of hypertension for 5 years. There was a sudden onset of left limbs weakness and slurred speech. The assessment of muscle strength was left limbs graded 0 and right limbs graded 5. NIHSS on admission was 10 points. The time of onset to admission was 1 h 24 min. A quick imaging evaluation verified the acute ischemic stroke caused by the right internal carotid artery (ICA) occlusion. Endovascular treatment was administered. After the long sheath (6 F, 90 cm) placed in the right femoral artery, an intermediate catheter (6 F, 105 cm, Navein) was brought into the ICA. Angiography showed the occlusion of the T terminal of ICA. Then assisted by micro guiding wire, the intermediate catheter was brought and reached the thrombus and absorbed by the Penumbra system. After one trial of a direct first pass aspiration technique (ADAPT), some of the thrombus were removed and the anterior cerebral artery (ACA) and proximal of the middle cerebral artery (MCA) were recanalized. Next, two trials of Solumbra technique using the Solitare FR (4 X 20 mm) were conducted and a complete recanalization (TICI 2b) was achieved (Figure 3). During the hospitalization, CT scan and MRI showed a hemorrhage infiltration in the right basal ganglia (Figure 3). Holter showed a sinus rhythm with atrial premature beat. But a single ECG examination detect a paroxysmal atrial fibrillation. This patient was charged five days after operation. Follow-up in 3months showed there was no another stroke attack and a good functional outcome with a mRS of 2.
Discussion
We listed three patients with acute ischemic stroke after video-assisted thoracic surgery transferred from the one chest hospital in our district. These patients were all subjected large vessel occluded stroke due to thrombus embolism. They underwent emergent endovascular treatment and had good outcomes in the follow up. Postoperative stroke is associated with high rates of mortality and disability. Although most of them are clinically unrecognized stroke, epidemiologic data shows that the incidence of perioperative stroke is 7% of noncardiac surgery elder patients [1]. Older age and previous cerebrovascular disease history are the most commonly and strongly identified risk factors for postoperative stroke [17]. Early data reports that incidence of perioperative ischemic stroke occurred in the early period during hospitalization after lobectomy was 0.6% [5]. Perioperative stroke was mainly attributed to embolic events, mostly in large vascular areas [8]. Although MT has been recommended for the first line treatment for LVO-AIS of the anterior circulation, there is still lack of the verification of its application on large number of cases of postoperative stroke. For these embolic stroke cases after video-assisted thoracic surgery, they are all relatively severer than ischemic stroke caused by intracerebral artery stenosis. It’s more urgent to have the vessels recanalized and restored of reperfusion. Since patients are always faint after thoracic surgery, the symptoms of stroke like limb weakness are easy to be neglected. It’s more challenging for patients to be identified and transferred to the stroke center in time. Due to wakeup stroke, the time of onset to reperfusion were much longer for case 1 than case 2 and case 3.
Strategy for stroke prevention is based on the identification of thrombus source. Thrombus formation in the pulmonary vein stump (PVS) [2,4,10,11,15,16], atrial fibrillation and vascular endothelial injury, fat embolism [13], air embolism [3] during procedure may contribute to the cerebral infarction after thoracic surgery. In our study, the first three patients all suffered embolic thrombus verified by angiography. Patient 1 is a young female without cardiogenic embolus and right to left shunt. The time of stroke onset after operation is relatively short indicated that vascular endothelial injury maybe the probable cause of thrombus formation. Therefore, anticoagulation was administrated for the probable pulmonary venous thrombosis. Patient 2 has a three-day period between operation and stroke onset, and the etiology of stroke is undermined since there is no clue of cardiogenic embolus. Antiplatelet drug was given because no benefit from anticoagulation for cryptogenic stroke. Maybe repeated and dynamic electrocardiogram monitoring is needed to detect potential arrhythmia for this patient. Although patient 3 has history of smoking and hypertension, the arteriosclerotic intracerebral artery stenosis was excluded in the angiography. The newly detected paroxysmal atrial fibrillation after operation suggested the probably cardiogenic embolus of stroke and anticoagulation therapy after MT
This case series shows the good effect of emergent endovascular treatment for cerebral embolism after thoracoscopic pulmonary intervention, suggesting that for such kind of patients, more attention should be paid to screen the risk factors of stroke before operation, to closely monitor neurological function after operation. Once postoperative stroke is suspected, it is very important to make an accurate diagnosis and take rapid vascular recanalization treatment to improve the prognosis.
Declarations
Competing interests: The authors declare that they have no competing interests.
Ethics Approval and Consent to Participate: This study was approved by the Ethics Committee of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital. The need for informed consent was approved by the Ethics Committee.
References
- Perioperative covert stroke in patients undergoing non-cardiac surgery (NeuroVISION): a prospective cohort study. Lancet. 2019; 394: 1022-1029
- Binbin Z, Yutao W, Chengwei Z. Postoperative Cerebral Embolism After video-assisted thoracoscopic left upper lobectomy : A Case Report and Literature Review. J Stroke Cerebrovasc Dis. 2019; 28: e139-e142
- Chen Y, Zheng C, Zeng Q, Zhang F, Tu S, Wu Z. Cerebral Air Embolism After Pigtail Catheter Drainage for Pneumothorax: A Case Report and Review of the Literature. Front Surg. 2021; 8: 743051
- Gual-Capllonch F, Teis A, Palomeras E. Pulmonary vein spontaneous echocontrast and stroke after pulmonary lobectomy. J Clin Ultrasound. 2013; 41: 321-322
- Jubelt B, Mihai C, Li TM, Veerapaneni P. Rhombencephalitis/ brainstem encephalitis. Curr Neurol Neurosci Rep. 2011; 11: 543-552
- Kimura D, Fukuda I, Tsushima T, Sakai T, Umetsu S, Ogasawara Y, Shimamura N, Ohkuma H. Management of acute ischemic stroke after pulmonary resection: incidence and efficacy of endovascular thrombus aspiration. Gen Thorac Cardiovasc Surg. 2019; 67: 306-311
- Leary MC, Varade P. Perioperative Stroke. Curr Neurol Neurosci Rep. 2020; 20: 12
- Meng L, Li J, Flexman AM, Tong C, Zhou X, Gelb AW, et al. Perceptions of Perioperative Stroke Among Chinese Anesthesiologists: Starting a Long March to Eliminate This Underappreciated Complication. Anesth Analg. 2019; 128:191-196
- Morinaga Y, Nii K, Sakamoto K, Inoue R, Mitsutake T, Hanada H. Revascularization for In-Hospital Acute Ischemic Stroke After Video-Assisted Thoracic Surgery: Report of 2 Cases and Literature Review. World Neurosurg. 2019; 129: 28-33
- Nakano T, Inaba M, Kaneda H. Recurrent cerebral attack caused by thrombosis in the pulmonary vein stump in a patient with left upper lobectomy on anticoagulant therapy: case report and literature review. Surg Case Rep. 2017; 3: 101
- Ohtaka K, Hida Y, Kaga K, Kato T, Muto J, Nakada-Kubota R, et al. Thrombosis in the pulmonary vein stump after left upper lobectomy as a possible cause of cerebral infarction. Ann Thorac Surg. 2013; 95: 1924-1928
- Saltman AP, Silver FL, Fang J, Stamplecoski M, Kapral MK. Care and Outcomes of Patients With In-Hospital Stroke. JAMA Neurol. 2015; 72: 749-755
- Scarpino M, Lanzo G, Cappelli F, Moretti M, Misuri G, Voltolini L, et al. Cerebral Fat Embolism After Video-Assisted Thoracic Surgery. Ann Thorac Surg. 2016; 102: e409-e411
- Shiozaki E, Morofuji Y, Kawahara I, Tagawa T, Tsutsumi K. Successful Endovascular Treatment for Middle Cerebral Artery Occlusion Caused by the Thrombus Formation in the Pulmonary Vein Stump Following Left Upper Lung Lobectomy. Cureus. 2021; 13: e17150
- Song CY, Kimura D, Sato F, Sakai T, Tsushima T, Fukuda I. Left superior pulmonary vein stump thrombosis and right renal infarction after left upper lobectomy: case report and literature review. Gen Thorac Cardiovasc Surg. 2020; 68: 1047-1050
- Usui G, Takayama Y, Hashimoto H, Katano T, Yanagiya M, Kusakabe M, et al. Cerebral Embolism Caused by Thrombus in the Pulmonary Vein Stump after Left Lower Lobectomy: A Case Report and Literature Review. Intern Med. 2019; 58: 1349-1354
- Vlisides PE, Moore LE. Stroke in Surgical Patients. Anesthesiology. 2021; 134: 480-492